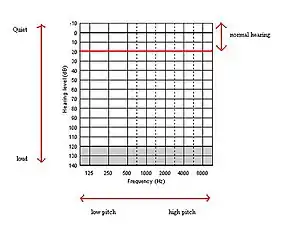
An audiogram is a graph that shows the audible threshold for standardized frequencies as measured by an audiometer. The Y axis represents intensity measured in decibels (dB) and the X axis represents frequency measured in hertz (Hz).[1] The threshold of hearing is plotted relative to a standardised curve that represents 'normal' hearing, in dB(HL). They are not the same as equal-loudness contours, which are a set of curves representing equal loudness at different levels, as well as at the threshold of hearing, in absolute terms measured in dB SPL (sound pressure level).
The frequencies displayed on the audiogram are octaves, which represent a doubling in frequency (e.g., 250 Hz, 500 Hz, 1000 Hz, wtc). Commonly tested "inter-octave" frequenices (e.g., 3000 Hz) may also be displayed. The intensities displayed on the audiogram appear as linear 10 dBHL steps. However, decibels are a logarithimic scale, so that successive 10 dB increments represent greater increases in loudness.
For humans, normal hearing is between −10 dB(HL) and 15 dB(HL),[2][3] although 0 dB from 250 Hz to 8 kHz is deemed to be 'average' normal hearing.
Hearing thresholds of humans and other mammals can be found with behavioural hearing tests or physiological tests used in audiometry. For adults, a behavioural hearing test involves a tester who presents tones at specific frequencies (pitches) and intensities (loudnesses). When the testee hears the sound he or she responds (e.g., by raising a hand or pressing a button. The tester records the lowest intensity sound the testee can hear.
With children, an audiologist makes a game out of the hearing test by replacing the feedback device with activity-related toys such as blocks or pegs. This is referred to as conditioned play audiometry. Visual reinforcement audiometry is also used with children. When the child hears the sound, he or she looks in the direction the sound came from and are reinforced with a light and/or animated toy. A similar technique can be used when testing some animals but instead of a toy, food can be used as a reward for responding to the sound.
Physiological tests do not need the patient to respond (Katz 2002). For example, when performing the brainstem auditory evoked potentials the patient's brainstem responses are being measured when a sound is played into their ear, or otoacoustic emissions which are generated by a healthy inner ear either spontaneously or evoked by an outside stimulus. In the US, the NIOSH recommends that people who are regularly exposed to hazardous noise have their hearing tested once a year, or every three years otherwise.[4]
Measurement
Audiograms are produced using a piece of test equipment called an audiometer, and this allows different frequencies to be presented to the subject, usually over calibrated headphones, at any specified level. The levels are, however, not absolute, but weighted with frequency relative to a standard graph known as the minimum audibility curve which is intended to represent a 'normal' hearing. This is not the best threshold found for all subjects, under ideal test conditions, which is represented by around 0 Phon or the threshold of hearing on the equal-loudness contours, but is standardised in an ANSI standard to a level somewhat higher at 1 kHz.[5] There are several definitions of the minimal audibility curve, defined in different international standards, and they differ significantly, giving rise to differences in audiograms according to the audiometer used. The ASA-1951 standard for example used a level of 16.5 dB(SPL) at 1 kHz whereas the later ANSI-1969/ISO-1963 standard uses 6.5 dB(SPL), and it is common to allow a 10 dB correction for the older standard.
Audiograms and types of hearing loss
"Conventional" pure tone audiometry (testing frequencies up to 8 kHz) is the basic measure of hearing status.[6] For research purposes, or early diagnosis of age-related hearing loss, ultra-high frequency audiograms (up to 20 kHz), requiring special audiometer calibration and headphones, can be measured.[7]
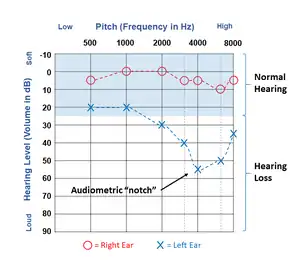
Different symbols indicate which ear the response is from and what type of response it is. Results of air conduction audiometry (in which the signals are presented to the ear through headphones, which create vibrations in the air) are reported using circles for the right ear and Xs for the left ear. Results of bone conduction audiometry (in which signals are presented using a vibrator which creates vibrations in the temporal bones of the head in order to bypass the outer and middle ear and test the inner ear and auditory nerve alone) are reporting using brackets. The open edge of the bracket indicates the ear tested, with < or [ representing a right bone conduction threshold and > or ] representing a left bone conduction threshold. When colors are used on an audiogram, red indicates the right ear and blue indicates the left ear.[8][9]
In adults, normal hearing is typically defined as thresholds of 25 dB HL or better (lower).[9] Thresholds of 30 dB HL and above indicate hearing loss.
The configuration of thresholds on an audiogram can often help determine the cause(s) of the hearing loss. For example, aging typically leads to hearing thresholds which get poorer as test frequencies get higher.[10] Noise induced hearing loss is typically characterized by a "notch" in the audiogram, with the poorest threshold occurring between 3000 and 6000 Hz (most often 4000 Hz) and better thresholds at lower and higher frequencies.[11]
Hearing impairment may also be the result of certain diseases such as CMV or Ménière's disease and these can be diagnosed from the shape of the audiogram. Otosclerosis results in an audiogram with significant loss at all frequencies, often of around 40 dB(HL).[12] A deficiency particularly around 2 kHz (termed a Carhart notch in the audiogram) is characteristic of either otosclerosis or a congenital ossicular anomaly.[13] Ménière's disease results in a severe loss at low frequencies.[14]
Constraints
Audiograms are unable to measure hidden hearing loss,[15][16] which is the inability to distinguish between sounds in loud environments such as restaurants. Hidden hearing loss is caused by synaptopathy in the cochlea,[17] as opposed to sensorineural hearing loss caused by hair cell dysfunction. Audiograms are designed to "estimate the softest sounds the patient can detect", and are not reflective of the loud situations that cause difficulties for people with hidden hearing loss. Audiograms may not reflect losses of nerve fibers that respond to loud sounds, key to understanding speech in noisy environments.[18] Research suggests a number of other measures, such as electrocochleography, speech-in-noise perception, and frequency following response, may be more useful.[17]
See also
References
- ↑ "What is an Audiogram?". www.babyhearing.org. babyhearing.org. Archived from the original on 8 March 2019. Retrieved 7 May 2018.
- ↑ Northern, Jerry L.; Downs, Marion P. (2002). Hearing in Children. Lippincott Williams & Wilkins. ISBN 9780683307641. Archived from the original on 2021-12-04. Retrieved 2020-11-24.
- ↑ Martin, Frederick N.; Clark, John Greer (2014). Introduction to Audiology (12 ed.). Pearson. ISBN 9780133491463.
- ↑ Noise and Hearing Loss Prevention: Frequently Asked Questions. Archived March 4, 2016, at the Wayback Machine NIOSH Safety and Health Topic.
- ↑ Sataloff, Robert Thayer; Sataloff, Joseph (1993). Hearing loss (3rd ed., rev. and expanded. ed.). New York: Dekker. ISBN 9780824790417.
- ↑ Roland, Peter (2004). Ototoxicity. BC Decker. p. 63. ISBN 978-1550092639.
The most commonly employed measure of auditory status is conventional audiometry (0.5-8 kHz).
- ↑ Conn, P. Michael (2011). Handbook of Models for Human Aging. Academic Press. p. 911. ISBN 978-0-12-369391-4.
For research purposes, or early diagnosis of presbycusis, ultra-high frequency audiograms can be measured. In such cases the test frequencies can go as high as 20 kHz and require special audiometer calibration and headphones.
- ↑ American Speech-Language-Hearing Association (1990). "Audiometric Symbols [Guidelines]". American Speech-Language-Hearing Association. Retrieved 2022-03-23.
- 1 2 Mroz, Mandy (2020-03-10). "How to read an audiogram". Healthy Hearing. Retrieved 2022-03-23.
- ↑ Cheslock, Megan; De Jesus, Orlando (2021-11-14), "Presbycusis", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 32644646, retrieved 2022-03-23
- ↑ Rabinowitz, Peter (2000-05-01). "Noise-Induced Hearing Loss". American Family Physician. 61 (9): 2749–2756. ISSN 0002-838X. PMID 10821155.
- ↑ pure tone audiometry in otosclerosis Archived 2008-12-08 at the Wayback Machine from General Practice Notebook. Retrieved 2012
- ↑ Kashio, A.; Ito, K.; Kakigi, A.; Karino, S.; Iwasaki, S. -I.; Sakamoto, T.; Yasui, T.; Suzuki, M.; Yamasoba, T. (2011). "Carhart Notch 2-kHz Bone Conduction Threshold Dip: A Nondefinitive Predictor of Stapes Fixation in Conductive Hearing Loss with Normal Tympanic Membrane". Archives of Otolaryngology–Head & Neck Surgery. 137 (3): 236–240. doi:10.1001/archoto.2011.14. PMID 21422306.
- ↑ pure tone audiometry in Meniere's disease Archived 2008-12-08 at the Wayback Machine from General Practice Notebook. Retrieved 2012
- ↑ Zheng, Fan-Gang (January 2015). "Uncovering Hidden Hearing Loss". The Hearing Journal. 68: 6. doi:10.1097/01.HJ.0000459741.56134.79. Archived from the original on December 13, 2020. Retrieved November 13, 2020.
- ↑ Liberman, M. Charles (August 2015). "Hidden Hearing Loss". Scientific American. 313 (2): 48–53. Bibcode:2015SciAm.313b..48L. doi:10.1038/scientificamerican0815-48. PMID 26349143. Archived from the original on 1 February 2021. Retrieved 13 December 2020.
- 1 2 Chen, Diyan; Jia, Gaogan; Ni, Yusu; Chen, Yan (June 2019). "Hidden hearing loss". Journal of Bio-X Research. 2 (2): 62–67. doi:10.1097/JBR.0000000000000035. ISSN 2096-5672. Archived from the original on 2021-12-04. Retrieved 2020-12-13.
- ↑ Blum, Haley (2017-07-01). "Lost in the Midst". The ASHA Leader. 22 (7): 48–55. doi:10.1044/leader.ftr1.22072017.48. Archived from the original on 2021-12-04. Retrieved 2020-12-13.
Further reading
- Gotfrit, M (1995) Range of human hearing [online] Available from https://web.archive.org/web/20160304000057/http://www.sfu.ca/sca/Manuals/ZAAPf/r/range.html Zen Audio Project [28th Feb 2007]
- Katz, J (2002)5th ed. Clinical Audiology Lippen-Cott Williams and Wilkins
- Rubel, E. Popper, A. Fay, R (1998) Development of the Auditory System New York: Springer-Verlag inc.