| Quinolone | |
|---|---|
| Drug class | |
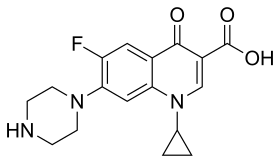 The second generation fluoroquinolone, ciprofloxacin. The two ringed nitrogen containing system with a ketone is called a quinolone. | |
| Class identifiers | |
| Use | Bacterial infection |
| ATC code | J01M |
| Clinical data | |
| Drugs.com | Drug Classes |
| External links | |
| MeSH | D015363 |
| Legal status | |
| In Wikidata | |
Quinolone antibiotics constitute a large group of broad-spectrum bacteriocidals that share a bicyclic core structure related to the substance 4-quinolone.[1] They are used in human and veterinary medicine to treat bacterial infections, as well as in animal husbandry, specifically poultry production.[2]
Nearly all quinolone antibiotics in use are fluoroquinolones, which contain a fluorine atom in their chemical structure and are effective against both Gram-negative and Gram-positive bacteria. One example is ciprofloxacin, one of the most widely used antibiotics worldwide.[3][4]
Medical uses
Fluoroquinolones are often used for genitourinary infections and are widely used in the treatment of hospital-acquired infections associated with urinary catheters. In community-acquired infections, they are recommended only when risk factors for multidrug resistance are present or after other antibiotic regimens have failed. However, for serious acute cases of pyelonephritis or bacterial prostatitis where the person may need to be hospitalised, fluoroquinolones are recommended as first-line therapy.[5]
Due to people with sickle-cell disease being at increased risk for developing osteomyelitis from the Salmonella, fluoroquinolones are the "drugs of choice" due to their ability to enter bone tissue without chelating it, as tetracyclines are known to do.
Fluoroquinolones are featured prominently in guidelines for the treatment of hospital-acquired pneumonia.[6]
Children
In most countries, fluoroquinolones are approved for use in children only under narrowly defined circumstances, owing in part to the observation of high rates of musculoskeletal adverse events in fluoroquinolone-treated juvenile animals. In the UK, the prescribing indications for fluoroquinolones for children are severely restricted. Only inhalant anthrax and pseudomonal infections in cystic fibrosis infections are licensed indications in the UK due to ongoing safety concerns. In a study comparing the safety and efficacy of levofloxacin to that of azithromycin or ceftriaxone in 712 children with community-acquired pneumonia, serious adverse events were experienced by 6% of those treated with levofloxacin and 4% of those treated with comparator antibiotics. Most of these were considered by the treating physician to be unrelated or doubtfully related to the study drug. Two deaths were observed in the levofloxacin group, neither of which was thought to be treatment-related. Spontaneous reports to the U.S. FDA Adverse Effects Reporting System at the time of the 20 September 2011 U.S. FDA Pediatric Drugs Advisory Committee included musculoskeletal events (39, including five cases of tendon rupture) and central nervous system events (19, including five cases of seizures) as the most common spontaneous reports between April 2005 and March 2008. An estimated 130,000 pediatric prescriptions for levofloxacin were filled on behalf of 112,000 pediatric patients during that period.[7]
Meta-analyses conclude that fluoroquinolones pose little or no additional risk to children compared to other antibiotic classes.[8][9][10] Fluoroquinolone use in children may be appropriate when the infection is caused by multidrug-resistant bacteria, or when alternative treatment options require parenteral administration and oral therapy is preferred.[11]
Adverse effects
While typical drug side effects reactions are mild to moderate, sometimes serious adverse effects occur.
Boxed warnings
In 2008, the U.S. FDA added black box warnings on all fluoroquinolones, advising of the increased risk of tendon damage.[12] In 2016, the FDA found that systemic use (by mouth or injection) of fluoroquinolones was associated with "disabling and potentially permanent serious side effects" involving the tendons, muscles, joints, nerves, and central nervous system, concluding that these side effects generally outweigh the benefits for people with acute sinusitis, acute bronchitis, and uncomplicated urinary tract infections when other treatment options are available.[13] Concerns regarding low blood sugar and mental health problems were added in 2018.[14]
Tendons
Quinolones are associated with a small risk of tendonitis and tendon rupture; a 2013 review found the incidence of tendon injury among those taking fluoroquinolones to be between 0.08 and 0.20%.[15] The risk appears to be higher among people older than 60 and those also taking corticosteroids;[15] the risk also may be higher among people who are male, have a pre-existing joint or tendon issue, have kidney disease, or are highly active.[16] Some experts have advised avoidance of fluoroquinolones in athletes.[16] If tendonitis occurs, it generally appears within one month, and the most common tendon injured appears to be the Achilles tendon.[15] The cause is not well understood.[15]
Nervous system
Nervous-system effects include insomnia, restlessness, and rarely, seizure, convulsions, and psychosis.[17] Other rare and serious adverse events have been observed with varying degrees of evidence for causation.[18][19][20][21]
Aortic dissection
Fluoroquinolones can increase the rate of rare but serious tears in the aorta by 31% compared to other antibiotics.[22] People at increased risk include those with aortic aneurysm, hypertension, certain genetic conditions such as Marfan syndrome and Ehlers-Danlos syndrome, and the elderly. For these people, fluoroquinolones should be used only when no other treatment options are available.[23]
Colitis
Clostridium difficile colitis may occur in connection with the use of any antibacterial drug, especially those with a broad spectrum of activity such as clindamycin, cephalosporins, and fluoroquinolones. Fluoroquinoline treatment is associated with risk that is similar to[24] or less than[25][26] that associated with broad spectrum cephalosporins. Fluoroquinoline administration may be associated with the acquisition and outgrowth of a particularly virulent Clostridium strain.[27]
Other
More generally, fluoroquinolones are tolerated, with typical drug side effects being mild to moderate.[28] Common side effects include gastrointestinal effects such as nausea, vomiting, and diarrhea, as well as headache and insomnia. Postmarketing surveillance has revealed a variety of relatively rare but serious adverse effects associated with all members of the fluoroquinolone antibacterial class. Among these, tendon problems and exacerbation of the symptoms of the neurological disorder myasthenia gravis are the subject of "black box" warnings in the United States.[29][30]
A 2018 EU-wide review of fluoroquinolones concluded that they are associated with serious side effects including tendonitis, tendon rupture, arthralgia, pain in extremities, gait disturbance, neuropathies associated with paraesthesia, depression, fatigue, memory impairment, sleep disorders, and impaired hearing, vision, taste and smell. Tendon damage (especially to Achilles tendon but also other tendons) can occur within 48 hours of starting fluoroquinolone treatment but the damage may be delayed several months after stopping treatment.[31]
The overall rate of adverse events in people treated with fluoroquinolones is roughly similar to that seen in people treated with other antibiotic classes.[25][32][33][34] A U.S. Centers for Disease Control and Prevention study found people treated with fluoroquinolones experienced adverse events severe enough to lead to an emergency department visit more frequently than those treated with cephalosporins or macrolides, but less frequently than those treated with penicillins, clindamycin, sulfonamides, or vancomycin.[35]
Fluoroquinolones prolong the heart's QT interval by blocking voltage-gated potassium channels.[36] Prolongation of the QT interval can lead to torsades de pointes, a life-threatening arrhythmia, but in practice, this appears relatively uncommon in part because the most widely prescribed fluoroquinolones (ciprofloxacin and levofloxacin) only minimally prolong the QT interval.[37]
In 2019 study by Journal of the American College of Cardiology it was discovered that fluoroquinolones could increase the risk for heart valve diseases.[38]
Events that may occur in acute overdose are rare, and include kidney failure and seizure.[39] Susceptible groups of patients, such as children and the elderly, are at greater risk of adverse reactions during therapeutic use.[28][40][41]
Mechanism of toxicity
The mechanisms of the toxicity of fluoroquinolones have been attributed to their interactions with different receptor complexes, such as blockade of the GABAA receptor complex within the central nervous system, leading to excitotoxic type effects[30] and oxidative stress.[42]
Interactions
Products containing multivalent cations, such as aluminium- or magnesium-containing antacids, and products containing calcium, iron, or zinc invariably result in marked reduction of oral absorption of fluoroquinolones.[43] Other drugs that interact with fluoroquinolones include sucralfate, probenecid, cimetidine, theophylline, warfarin, antiviral agents, phenytoin, cyclosporine, rifampin, pyrazinamide, and cycloserine.[43]
Administration of quinolone antibiotics to a benzodiazepine-dependent individual can precipitate acute benzodiazepine withdrawal symptoms due to quinolones displacing benzodiazepines from their binding sites.[44] Fluoroquinolones have varying specificity for cytochrome P450, so may have interactions with drugs cleared by those enzymes; the order from most P450-inhibitory to least, is enoxacin > ciprofloxacin > norfloxacin > ofloxacin, levofloxacin, trovafloxacin, gatifloxacin, moxifloxacin.[43]
Contraindications
Quinolones are not recommended in people with epilepsy, Marfan's syndrome, Ehlers-Danlos Syndrome,[45] QT prolongation, pre-existing CNS lesions, or CNS inflammation, or who have had a stroke.[30] They are best avoided in the athlete population.[46] Safety concerns exist for fluoroquinolone use during pregnancy, so they are contraindicated unless no other safe alternative antibiotic exists.[47] However, one meta-analysis looking at the outcome of pregnancies involving quinolone use in the first trimester found no increased risk of malformations.[48] They are also contraindicated in children due to the risks of damage to the musculoskeletal system.[49] Their use in children is not absolutely contraindicated, however. For certain severe infections where other antibiotics are not an option, their use can be justified.[50] Quinolones should also not be given to people with a known hypersensitivity to the drug class.[51][52]
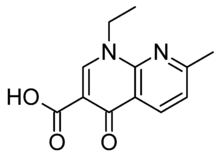
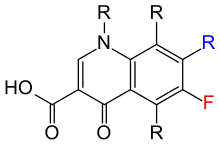
The basic pharmacophore, or active structure, of the fluoroquinolone class is based upon the quinoline ring system.[53] The addition of the fluorine atom at C6 distinguishes the successive-generation fluoroquinolones from the first-generation of quinolones. The addition of the C6 fluorine atom has since been demonstrated not to be required for the antibacterial activity of this class (circa 1997).[54]
Antibiotic misuse and bacterial resistances
Because the use of broad-spectrum antibiotics encourages the spread of multidrug-resistant strains and the development of Clostridium difficile infections, treatment guidelines often recommend minimizing the use of fluoroquinolones and other broad-spectrum antibiotics in less severe infections and in those in which risk factors for multidrug resistance are not present. It has been recommended that fluoroquinolones not be used as a first-line agent for community-acquired pneumonia,[55] instead recommending macrolide or doxycycline as first-line agents. The Drug-Resistant Streptococcus pneumoniae Working Group recommends fluoroquinolones be used for the ambulatory treatment of community-acquired pneumonia only after other antibiotic classes have been tried and failed, or in cases with demonstrated drug-resistant Streptococcus pneumoniae.[56]
Resistance to quinolones can evolve rapidly, even during a course of treatment. Numerous pathogens, including Escherichia coli, commonly exhibit resistance.[57] Widespread veterinary usage of quinolones, in particular in Europe, has been implicated.[58]
Fluoroquinolones had become the class of antibiotics most commonly prescribed to adults in 2002. Nearly half (42%) of these prescriptions were for conditions not approved by the U.S. FDA, such as acute bronchitis, otitis media, and acute upper respiratory tract infection, according to a study supported in part by the Agency for Healthcare Research and Quality.[59][60] In addition, they are commonly prescribed for medical conditions, such as acute respiratory illness, that are usually caused by viral infections.[61]
Three mechanisms of resistance are known.[62] Some types of efflux pumps can act to decrease intracellular quinolone concentration.[63] In gram-negative bacteria, plasmid-mediated resistance genes produce proteins that can bind to DNA gyrase, protecting it from the action of quinolones. Finally, mutations at key sites in DNA gyrase or topoisomerase IV can decrease their binding affinity to quinolones, decreasing the drugs' effectiveness.
Mechanism of action
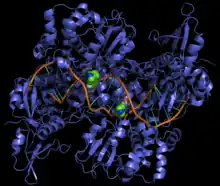
Quinolones are chemotherapeutic bactericidal drugs. They interfere with DNA replication by preventing bacterial DNA from unwinding and duplicating.[64] Specifically, they inhibit the ligase activity of the type II topoisomerases, DNA gyrase and topoisomerase IV, which cut DNA to introduce supercoiling, while leaving nuclease activity unaffected. With the ligase activity disrupted, these enzymes release DNA with single- and double-strand breaks that lead to cell death.[65] The majority of quinolones in clinical use are fluoroquinolones, which have a fluorine atom attached to the central ring system, typically at the 6-position or C-8 position. Most of them are named with the -oxacin suffix. First and second generation quinolones are largely active against Gram-negative bacteria, whereas third and fourth generation quinolones have increased activity against Gram-positive and anaerobic bacteria.[66] Some quinolones containing aromatic substituents at their C-7 positions are highly active against eukaryotic type II topoisomerase.[67]
It has also been proposed that quinolone antibiotics cause oxidation of guanine nucleotides in the bacterial nucleotide pool, and that this process contributes to the cytotoxicity of these agents.[68] The incorporation of oxidized guanine nucleotides into DNA could be bactericidal. Bacterial cytotoxicity could arise from incomplete repair of closely spaced 8-oxo-2'-deoxyguanosine in the DNA resulting in double-strand breaks.[68]
Cellular uptake
Fluoroquinolones can enter in cells easily via porins, so are often used to treat intracellular pathogens such as Legionella pneumophila and Mycoplasma pneumoniae. For many Gram-negative bacteria, DNA gyrase is the target, whereas topoisomerase IV is the target for many Gram-positive bacteria.
Eukaryotic cells are not believed to contain DNA gyrase or topoisomerase IV. However, debate exists concerning whether the quinolones still have such an adverse effect on the DNA of healthy cells. Some compounds in this class have been shown to inhibit the synthesis of mitochondrial DNA.[69][70][71][72]
Pharmacology
The basic pharmacophore, or active structure, of the fluoroquinolone class is based upon the quinoline ring system.[73] Various substitutions made to the quinoline ring resulted in the development of numerous fluoroquinolone drugs. The addition of the fluorine atom at C-6 distinguishes the successive-generation fluoroquinolones from the first-generation quinolones, although examples are known that omit the atom while retaining antibacterial activity.[54]
Pharmacokinetics
| Drug | Dosagea (mg) | BA (%) | Cmax (μg/mL) | tmax (h) | AUC (μg • h/mL) | t1/2 (h) | Vd/F (L/kg) | Protein binding (%) | Excreted unchanged (%) | Dose adjustment | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Renal | Hepatic | ||||||||||
| Ciprofloxacin | 500 750 | 70 70 | 2.30 3.00 | 1.2 1.2 | 10.1 14.0 | 3.5 3.5 | 3.5 3.5 | 30 30 | 34 34 | Yes Yes | No No |
| Garenoxacin | 400 600 | ND 92 | 5.0 10.4 | ND 1.2 | 60 96.7 | 14.2 9.8 | ND ND | 75 ND | 40 ND | ND ND | ND ND |
| Gatifloxacin | 400 | 96 | 3.86 | 1.5 | 33.8 | 8.0 | 1.8 | 20 | 76 | Yes | No |
| Gemifloxacin | 320 640 | 70 70 | 1.19 2.29 | 1.2 1.2 | 7.3 15.9 | 8.0 8.0 | 3.5 3.5 | 60 60 | 27 27 | Yes Yes | No No |
| Levofloxacin | 500 750 | 99 99 | 5.08 7.13 | 1.7 1.7 | 48.0 82.0 | 6.9 6.9 | 1.1 1.1 | 31 31 | 83 83 | Yes Yes | ND ND |
| Moxifloxacin | 200 400 | 86 86 | 1.16 3.34 | 1.7 1.7 | 15.4 33.8 | 12.1 12.1 | 3.3 3.3 | 47 47 | 19 19 | No No | No No |
| a = Dosage applies only to Cmax and AUC. The other parameters an average of the values available in the literature irrespective of dosage. | |||||||||||
History
Although not formally a quinolone, nalidixic acid is considered the first quinolone drug. It was introduced in 1962 for treatment of urinary tract infections (UTIs) in humans.[75] Nalidixic acid was discovered by George Lesher and coworkers in a distillate during an attempt at chloroquine synthesis.[76] Nalidixic acid is thus considered to be the predecessor of all members of the quinolone family, including the second, third and fourth generations commonly known as fluoroquinolones. Since the introduction of nalidixic acid, more than 10,000 analogs have been synthesized, but only a handful have found their way into clinical practice. The first generation also included other quinolone drugs, such as pipemidic acid, oxolinic acid, and cinoxacin, which were introduced in the 1970s. They proved to be only marginal improvements over nalidixic acid.[77]
These drugs were widely used as a first-line treatment for many infections, including very commons ones such as acute sinusitis, acute bronchitis, and uncomplicated UTIs.[78] Reports of serious adverse events began emerging, and the FDA first added a black-box warning to fluoroquinolones in July 2008 for the increased risk of tendinitis and tendon rupture. In February 2011, the risk of worsening symptoms for those with myasthenia gravis was added to the warning. In August 2013, the agency required updates to the labels to describe the potential for irreversible peripheral neuropathy (serious nerve damage).
In November 2015, an FDA Advisory Committee discussed the risks and benefits of fluoroquinolones for the treatment of acute bacterial sinusitis, acute bacterial exacerbation of chronic bronchitis, and uncomplicated UTIs based on new safety information. The new information focused on two or more side effects occurring at the same time and causing the potential for irreversible impairment. The advisory committee concluded that the serious risks associated with the use of fluoroquinolones for these types of uncomplicated infections generally outweighed the benefits for patients with other treatment options.[78][79][80][81][82] The 21-member joint committee overwhelmingly recommended stronger label warnings on the containers because of rare but sometimes devastating side effects.[83]
On 12 May 2016, the FDA issued a drug safety communication advising that fluoroquinolones should be reserved for these conditions only when no other options are available due to potentially permanent, disabling side effects occurring together. The drug safety communication also announced the required labeling updates to reflect this new safety information.[78] The FDA put out another label change in July 2017, strengthening the warnings about potentially disabling adverse effects and limiting use of these drugs to second-line treatments for acute sinusitis, acute bronchitis, and uncomplicated UTIs.[78]
Generations
The first generation of the quinolones began following introduction of the related, but structurally distinct naphthyridine-family nalidixic acid in 1962 for treatment of UTIs in humans.[84] Nalidixic acid was discovered by George Lesher and coworkers in a chemical distillate during an attempt at synthesis of the chloroquinoline antimalarial agent, chloroquine.[85] Naphthyridone and quinolone classes of antibiotics prevent bacterial DNA replication by inhibition of DNA unwinding events, and can be both bacteriostatic and bacteriocidal.[64] (See Mechanism of Action later.) The majority of quinolones in clinical use belong to the second generation class of "fluoroquinolones", which have a true quinoline framework, maintain the C-3 carboxylic acid group, and add a fluorine atom to the all-carbon containing ring, typically at the C-6 or C-8 positions. [66]
Quinolones can be classified into generations based on their antibacterial spectrums.[86][87] The earlier-generation agents are, in general, more narrow-spectrum than the later ones, but no standard is employed to determine which drug belongs to which generation. The only universal standard applied is the grouping of the non-fluorinated drugs found within this class (quinolones) within the first-generation heading. As such, a wide variation exists within the literature dependent upon the methods employed by the authors.
The first generation is rarely used. Frequently prescribed drugs are moxifloxacin, ciprofloxacin, levofloxacin.
First generation
- flumequine (veterinary use)
- oxolinic acid
- rosoxacin
Structurally related first-generation drugs, but formally not 4-quinolones, include cinoxacin,[88] nalidixic acid,[88] and piromidic acid, pipemidic acid
Second generation
The second-generation class is sometimes subdivided into "Class 1" and "Class 2".[88]
- ciprofloxacin[88][89]
- fleroxacin
- lomefloxacin[88]
- nadifloxacin
- norfloxacin
- ofloxacin[88]
- pefloxacin
- rufloxacin
A structurally related second-generation drug, but formally not a 4-quinolone, is enoxacin.[88]
Third generation
Unlike the first and second generations, the third generation is active against streptococci.[88]
A structurally related third-generation drug, but formally not a 4-quinolone, is tosufloxacin (Ozex, Tosacin).
Fourth generation
Fourth-generation fluoroquinolones act at DNA gyrase and topoisomerase IV.[91] This dual action slows development of resistance.
- clinafloxacin[89]
- gatifloxacin[92]
- moxifloxacin[88]
- sitafloxacin
- prulifloxacin
- besifloxacin
- delafloxacin
Two structurally related third-generation drugs, but formally not 4-quinolones, are gemifloxacin and trovafloxacin (removed from clinical use).[88][89]
In development:
Veterinary use
Quinolones have been widely used in animal husbandry, and several agents have veterinary-specific applications.
- danofloxacin – 2nd gen, related to ciprofloxacin
- difloxacin – 2nd/3rd gen, related to temafloxacin
- enrofloxacin – 2nd gen, metabolizes into ciprofloxacin
- ibafloxacin – 3rd gen, related to levofloxacin
- marbofloxacin – 3rd gen, related to levofloxacin
- orbifloxacin – 3rd gen, related to sparfloxacin
- sarafloxacin – 2nd/3rd gen, related to difloxacin
References
![]() This article incorporates public domain material from FDA updates warnings for fluoroquinolone antibiotics. United States Department of Health and Human Services.
This article incorporates public domain material from FDA updates warnings for fluoroquinolone antibiotics. United States Department of Health and Human Services.
- ↑ Andriole, VT The Quinolones. Academic Press, 1989.
- ↑ Johnson, James R.; Murray, Andrew C.; Gajewski, Abby; Sullivan, Maureen; Snippes, Paula; Kuskowski, Michael A.; Smith, Kirk E. (2003). "Isolation and Molecular Characterization of Nalidixic Acid-Resistant Extraintestinal Pathogenic Escherichia coli from Retail Chicken Products". Antimicrobial Agents and Chemotherapy. 47 (7): 2161–2168. doi:10.1128/AAC.47.7.2161-2168.2003. PMC 161843. PMID 12821463.
- ↑ Andersson MI, MacGowan AP (May 2003). "Development of the quinolones". The Journal of Antimicrobial Chemotherapy. 51 Suppl 1 (Suppl. S1): 1–11. doi:10.1093/jac/dkg212. PMID 12702698.
- ↑ Heeb S, Fletcher MP, Chhabra SR, Diggle SP, Williams P, Cámara M (March 2011). "Quinolones: from antibiotics to autoinducers". FEMS Microbiology Reviews. 35 (2): 247–74. doi:10.1111/j.1574-6976.2010.00247.x. PMC 3053476. PMID 20738404.
- ↑ Liu H, Mulholland SG (July 2005). "Appropriate antibiotic treatment of genitourinary infections in hospitalized patients". The American Journal of Medicine. 118 Suppl 7A (7): 14S–20S. doi:10.1016/j.amjmed.2005.05.009. PMID 15993673.
- ↑ Infectious Diseases Society of America (February 2005). "Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia". American Journal of Respiratory and Critical Care Medicine. 171 (4): 388–416. doi:10.1164/rccm.200405-644ST. PMID 15699079. S2CID 14907563.
- ↑ "Adverse Event Review: Levaquin® (levofloxacin): Pediatric Advisory Committee Meeting" (PDF). Food and Drug Administration. 18 November 2008.
- ↑ Sung L, Manji A, Beyene J, et al. (May 2012). "Fluoroquinolones in children with fever and neutropenia: a systematic review of prospective trials". The Pediatric Infectious Disease Journal. 31 (5): 431–5. doi:10.1097/INF.0b013e318245ab48. PMID 22189521. S2CID 52835801.
- ↑ Rosanova MT, Lede R, Capurro H, Petrungaro V, Copertari P (December 2010). "[Assessing fluoroquinolones as risk factor for musculoskeletal disorders in children: a systematic review and meta-analysis]". Archivos Argentinos de Pediatria (in Spanish). 108 (6): 524–31. doi:10.1590/S0325-00752010000600008 (inactive 1 August 2023). PMID 21132249.
{{cite journal}}: CS1 maint: DOI inactive as of August 2023 (link) - ↑ Forsythe CT, Ernst ME (November 2007). "Do fluoroquinolones commonly cause arthropathy in children?". Canadian Journal of Emergency Medicine. 9 (6): 459–62. doi:10.1017/s1481803500015517. PMID 18072993.
- ↑ Bradley JS, Jackson MA (October 2011). "The use of systemic and topical fluoroquinolones". Pediatrics. 128 (4): e1034-45. doi:10.1542/peds.2011-1496. PMID 21949152.
- ↑ "FDA orders 'black box' label on some antibiotics". CNN. 8 July 2008. Retrieved 8 July 2008.
- ↑ "FDA Drug Safety Communication: FDA advises restricting fluoroquinolone antibiotic use for certain uncomplicated infections; warns about disabling side effects that can occur together". FDA. 12 May 2016.
- ↑ "Safety Alerts for Human Medical Products - Fluoroquinolone Antibiotics: FDA Requires Labeling Changes Due to Low Blood Sugar Levels and Mental Health Side Effects". www.fda.gov. Retrieved 13 July 2018.
- 1 2 3 4 Stephenson AL, Wu W, Cortes D, Rochon PA (September 2013). "Tendon Injury and Fluoroquinolone Use: A Systematic Review". Drug Safety. 36 (9): 709–21. doi:10.1007/s40264-013-0089-8. PMID 23888427. S2CID 24948660.
- 1 2 Lewis T, Cook J (2014). "Fluoroquinolones and tendinopathy: a guide for athletes and sports clinicians and a systematic review of the literature". Journal of Athletic Training. 49 (3): 422–7. doi:10.4085/1062-6050-49.2.09. PMC 4080593. PMID 24762232.
- ↑ Galatti L, Giustini SE, Sessa A, et al. (March 2005). "Neuropsychiatric reactions to drugs: an analysis of spontaneous reports from general practitioners in Italy". Pharmacological Research. 51 (3): 211–6. doi:10.1016/j.phrs.2004.08.003. PMID 15661570.
- ↑ Babar S (October 2013). "SIADH Associated With Ciprofloxacin". The Annals of Pharmacotherapy. 47 (10): 1359–1363. doi:10.1177/1060028013502457. ISSN 1060-0280. PMID 24259701. S2CID 36759747.
- ↑ Rouveix B (November–December 2006). "[Clinically significant toxicity and tolerance of the main antibiotics used in lower respiratory tract infections]". Médecine et Maladies Infectieuses. 36 (11–12): 697–705. doi:10.1016/j.medmal.2006.05.012. PMID 16876974.
- ↑ Mehlhorn AJ, Brown DA (November 2007). "Safety concerns with fluoroquinolones". The Annals of Pharmacotherapy. 41 (11): 1859–66. doi:10.1345/aph.1K347. PMID 17911203. S2CID 26411679.
- ↑ Jones SF, Smith RH (March 1997). "Quinolones may induce hepatitis". The BMJ. 314 (7084): 869. doi:10.1136/bmj.314.7084.869. PMC 2126221. PMID 9093098.
- ↑ Newton ER, Akerman AW, Strassle PD, Kibbe MR (January 2021). "Association of Fluoroquinolone Use With Short-term Risk of Development of Aortic Aneurysm". JAMA Surgery. 156 (3): 264–272. doi:10.1001/jamasurg.2020.6165. PMC 7788511. PMID 33404647.
- ↑ "FDA warns about increased risk of ruptures or tears in the aorta blood vessel with fluoroquinolone antibiotics in certain patients". FDA. 20 December 2018. Retrieved 9 February 2019.
- ↑ Deshpande A, Pasupuleti V, Thota P, et al. (September 2013). "Community-associated Clostridium difficile infection and antibiotics: a meta-analysis". Journal of Antimicrobial Chemotherapy. 68 (9): 1951–61. doi:10.1093/jac/dkt129. PMID 23620467.
- 1 2 Levine JG, Szarfman A (15 December 2006). "Data Mining Analysis of Multiple Antibiotics in AERS" (Microsoft PowerPoint). Food and Drug Administration.
{{cite journal}}: Cite journal requires|journal=(help) - ↑ Slimings C, Riley TV (December 2013). "Antibiotics and hospital-acquired Clostridium difficile infection: update of systematic review and meta-analysis". Journal of Antimicrobial Chemotherapy. 69 (4): 881–891. doi:10.1093/jac/dkt477. PMID 24324224.
- ↑ Vardakas KZ, Konstantelias AA, Loizidis G, Rafailidis PI, Falagas ME (November 2012). "Risk factors for development of Clostridium difficile infection due to BI/NAP1/027 strain: a meta-analysis". International Journal of Infectious Diseases. 16 (11): e768–73. doi:10.1016/j.ijid.2012.07.010. PMID 22921930.
- 1 2 Owens RC, Ambrose PG (July 2005). "Antimicrobial safety: focus on fluoroquinolones". Clinical Infectious Diseases. 41 (Suppl 2): S144–57. doi:10.1086/428055. PMID 15942881.
- ↑ "Information for Healthcare Professionals: Fluoroquinolone Antimicrobial Drugs [ciprofloxacin (Marketed as Cipro and generic ciprofloxacin), ciprofloxacin extended-release (Marketed as Cipro XR and Proquin XR), gemifloxacin (Marketed as Factive), levofloxacin (Marketed as Levaquin), moxifloxacin (Marketed as Avelox), norfloxacin (Marketed as Noroxin), and ofloxacin (Marketed as Floxin)]". Food and Drug Administration. Archived from the original on 30 October 2017. Retrieved 16 December 2019.
- 1 2 3 De Sarro A, De Sarro G (March 2001). "Adverse reactions to fluoroquinolones. an overview on mechanistic aspects". Current Medicinal Chemistry. 8 (4): 371–84. doi:10.2174/0929867013373435. PMID 11172695.
- ↑ "Disabling and potentially permanent side effects lead to suspension or restrictions of quinolone and fluoroquinolone antibiotics". European Medicines Agency. 11 March 2019.
- ↑ Skalsky K, Yahav D, Lador A, Eliakim-Raz N, Leibovici L, Paul M (April 2013). "Macrolides vs. quinolones for community-acquired pneumonia: meta-analysis of randomized controlled trials". Clinical Microbiology and Infection. 19 (4): 370–8. doi:10.1111/j.1469-0691.2012.03838.x. PMID 22489673.
- ↑ Falagas ME, Matthaiou DK, Vardakas KZ (December 2006). "Fluoroquinolones vs beta-lactams for empirical treatment of immunocompetent patients with skin and soft tissue infections: a meta-analysis of randomized controlled trials". Mayo Clinic Proceedings. 81 (12): 1553–66. doi:10.4065/81.12.1553. PMID 17165634.
- ↑ Van Bambeke F, Tulkens PM (2009). "Safety profile of the respiratory fluoroquinolone moxifloxacin: comparison with other fluoroquinolones and other antibacterial classes". Drug Safety. 32 (5): 359–78. doi:10.2165/00002018-200932050-00001. PMID 19419232. S2CID 19026852.
- ↑ Shehab N, Patel PR, Srinivasan A, Budnitz DS (September 2008). "Emergency department visits for antibiotic-associated adverse events". Clinical Infectious Diseases. 47 (6): 735–43. doi:10.1086/591126. PMID 18694344.
- ↑ Heidelbaugh JJ, Holmstrom H (April 2013). "The perils of prescribing fluoroquinolones". The Journal of Family Practice. 62 (4): 191–7. PMID 23570031.
- ↑ Rubinstein E, Camm J (April 2002). "Cardiotoxicity of fluoroquinolones". Journal of Antimicrobial Chemotherapy. 49 (4): 593–6. doi:10.1093/jac/49.4.593. PMID 11909831.
- ↑ Bakalar, Nicholas (17 September 2019). "Antibiotics Tied to Heart Valve Problems". The New York Times. ISSN 0362-4331. Retrieved 24 August 2021.
- ↑ Nelson LH, Flomenbaum N, Goldfrank LR, Hoffman RL, Howland MD, Lewin NA (2006). Goldfrank's toxicologic emergencies. New York: McGraw-Hill, Medical Pub. Division. ISBN 978-0-07-143763-9.
- ↑ Iannini PB (June 2007). "The safety profile of moxifloxacin and other fluoroquinolones in special patient populations". Current Medical Research and Opinion. 23 (6): 1403–13. doi:10.1185/030079907X188099. PMID 17559736. S2CID 34091286.
- ↑ Farinas ER, et al. (Public Health Service Food and Drug Administration Center for Drug Evaluation and Research) (1 March 2005). "Consult: One-Year Post Pediatric Exclusivity Postmarketing Adverse Events Review" (PDF). Food and Drug Administration. Retrieved 31 August 2009.
- ↑ Saint F, Salomon L, Cicco A, de la Taille A, Chopin D, Abbou CC (December 2001). "[Tendinopathy associated with fluoroquinolones: individuals at risk, incriminated physiopathologic mechanisms, therapeutic management]". Progrès en Urologie (in French). 11 (6): 1331–4. PMID 11859676.
- 1 2 3 Fish DN (2001). "Fluoroquinolone Adverse Effects and Drug Interactions". Pharmacotherapy. 21 (10 Suppl): 253S–272S. doi:10.1592/phco.21.16.253S.33993. PMID 11642691. S2CID 29617455.
- ↑ Ford C, Law F (July 2014). "Guidance for the use and reduction of misuse of benzodiazepines and other hypnotics and anxiolytics in general practice" (PDF). SMMGP. Archived from the original (PDF) on 6 July 2017. Retrieved 24 July 2017.
{{cite journal}}: Cite journal requires|journal=(help) - ↑ "Fluoroquinolones Antibiotic Alert – especially with EDS". 29 August 2013.
- ↑ 2011 Documentlevaquinadversesideeffect.com Archived 17 June 2021 at the Wayback Machine
- ↑ Nardiello S, Pizzella T, Ariviello R (March 2002). "[Risks of antibacterial agents in pregnancy]". Le Infezioni in Medicina. 10 (1): 8–15. PMID 12700435.
- ↑ Bar-Oz B, Moretti ME, Boskovic R, O'Brien L, Koren G (April 2009). "The safety of quinolones--a meta-analysis of pregnancy outcomes". European Journal of Obstetrics, Gynecology, and Reproductive Biology. 143 (2): 75–8. doi:10.1016/j.ejogrb.2008.12.007. PMID 19181435.
- ↑ Noel GJ, Bradley JS, Kauffman RE, Duffy CM, Gerbino PG, Arguedas A, et al. (October 2007). "Comparative safety profile of levofloxacin in 2523 children with a focus on four specific musculoskeletal disorders". The Pediatric Infectious Disease Journal. 26 (10): 879–91. doi:10.1097/INF.0b013e3180cbd382. PMID 17901792. S2CID 26457648.
- ↑ Leibovitz E (February 2006). "The use of fluoroquinolones in children". Current Opinion in Pediatrics. 18 (1): 64–70. doi:10.1097/01.mop.0000192520.48411.fa. PMID 16470165. S2CID 37437573.
- ↑ Janssen Pharmaceutica (September 2008). "Highlights of Prescribing Information" (PDF). Food and Drug Administration.
- ↑ Scherer K, Bircher AJ (January 2005). "Hypersensitivity reactions to fluoroquinolones". Current Allergy and Asthma Reports. 5 (1): 15–21. doi:10.1007/s11882-005-0049-1. PMID 15659258. S2CID 31447696.
- ↑ Schaumann R, Rodloff AC (January 2007). "Activities of Quinolones Against Obligately Anaerobic Bacteria" (PDF). Anti-Infective Agents in Medicinal Chemistry. 6 (1): 49–56. doi:10.2174/187152107779314179. Archived from the original (PDF) on 16 June 2010. Retrieved 6 May 2011.
- 1 2 Hong CY, Kim SH, Kim YK (22 July 1997). "Novel 5-amino-6-methylquinolone antibacterials: A new class of non-6-fluoroquinolones". Bioorganic & Medicinal Chemistry Letters. 7 (14): 1875–1878. doi:10.1016/S0960-894X(97)00324-7.
- ↑ Mandell LA, Wunderink RG, Anzueto A, et al. (March 2007). "Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults". Clinical Infectious Diseases. 44 (Suppl 2): S27–72. doi:10.1086/511159. PMC 7107997. PMID 17278083.
- ↑ MacDougall C, Guglielmo BJ, Maselli J, Gonzales R (March 2005). "Antimicrobial drug prescribing for pneumonia in ambulatory care". Emerging Infectious Diseases. 11 (3): 380–4. doi:10.3201/eid1103.040819. PMC 3298265. PMID 15757551.
- ↑ M Jacobs, Worldwide Overview of Antimicrobial Resistance. International Symposium on Antimicrobial Agents and Resistance 2005.
- ↑ Nelson JM, Chiller TM, Powers JH, Angulo FJ (April 2007). "Fluoroquinolone-resistant Campylobacter species and the withdrawal of fluoroquinolones from use in poultry: a public health success story". Clinical Infectious Diseases. 44 (7): 977–80. doi:10.1086/512369. PMID 17342653.
- ↑ Linder JA, Huang ES, Steinman MA, Gonzales R, Stafford RS (March 2005). "Fluoroquinolone prescribing in the United States: 1995 to 2002". The American Journal of Medicine. 118 (3): 259–68. doi:10.1016/j.amjmed.2004.09.015. PMID 15745724.
- ↑ K08 HS14563 and HS11313
- ↑ Neuhauser MM, Weinstein RA, Rydman R, Danziger LH, Karam G, Quinn JP (February 2003). "Antibiotic resistance among gram-negative bacilli in US intensive care units: implications for fluoroquinolone use". JAMA. 289 (7): 885–8. doi:10.1001/jama.289.7.885. PMID 12588273.
From 1995 to 2002, inappropriate antibiotic prescribing for acute respiratory infections, which are usually caused by viruses and thus are not responsive to antibiotics, declined from 61 to 49 percent. However, the use of broad-spectrum antibiotics such as the fluoroquinolones, jumped from 41 to 77 percent from 1995 to 2001. Overuse of these antibiotics will eventually render them useless for treating antibiotic-resistant infections, for which broad-spectrum antibiotics are supposed to be reserved.
- ↑ Robicsek A, Jacoby GA, Hooper DC (October 2006). "The worldwide emergence of plasmid-mediated quinolone resistance". Lancet Infect. Dis. 6 (10): 629–40. doi:10.1016/S1473-3099(06)70599-0. PMID 17008172.
- ↑ Morita Y, Kodama K, Shiota S, Mine T, Kataoka A, Mizushima T, Tsuchiya T (July 1998). "NorM, a Putative Multidrug Efflux Protein, of Vibrio parahaemolyticus and Its Homolog in Escherichia coli". Antimicrobial Agents and Chemotherapy. 42 (7): 1778–82. doi:10.1128/AAC.42.7.1778. PMC 105682. PMID 9661020.
- 1 2 Hooper DC (March–April 2001). "Emerging mechanisms of fluoroquinolone resistance". Emerging Infectious Diseases. 7 (2): 337–41. doi:10.3201/eid0702.010239. PMC 2631735. PMID 11294736.
- ↑ Aldred KJ, Kerns RJ, Osheroff N (March 2014). "Mechanism of quinolone action and resistance". Biochemistry. 53 (10): 1565–74. doi:10.1021/bi5000564. PMC 3985860. PMID 24576155.
- 1 2 Andriole VT (July 2005). "The quinolones: past, present, and future". Clinical Infectious Diseases. 41 Suppl 2 (S2): S113-9. doi:10.1086/428051. PMID 15942877.
- ↑ Elsea SH, Osheroff N, Nitiss JL (July 1992). "Cytotoxicity of quinolones toward eukaryotic cells. Identification of topoisomerase II as the primary cellular target for the quinolone CP-115,953 in yeast" (PDF). The Journal of Biological Chemistry. 267 (19): 13150–3. doi:10.1016/S0021-9258(18)42185-0. PMID 1320012. Retrieved 6 May 2011.
- 1 2 Foti JJ, Devadoss B, Winkler JA, Collins JJ, Walker GC. Oxidation of the guanine nucleotide pool underlies cell death by bactericidal antibiotics. Science. 2012 Apr 20;336(6079):315-9. doi: 10.1126/science.1219192. PMID: 22517853; PMCID: PMC3357493
- ↑ Bergan T, Bayer (1988). Pharmacokinetics of fluorinated quinolones. Academic Press. pp. 119–154.
- ↑ Bergan T, Dalhoff A, Thorsteinsson SB (1985). "A review of the pharmacokinetics and tissue penetration of ciprofloxacin": 23–36.
{{cite journal}}: Cite journal requires|journal=(help) - ↑ Castora FJ, Vissering FF, Simpson MV (September 1983). "The effect of bacterial DNA gyrase inhibitors on DNA synthesis in mammalian mitochondria". Biochimica et Biophysica Acta (BBA) - Gene Structure and Expression. 740 (4): 417–27. doi:10.1016/0167-4781(83)90090-8. PMID 6309236.
- ↑ Suto MJ, Domagala JM, Roland GE, Mailloux GB, Cohen MA (December 1992). "Fluoroquinolones: relationships between structural variations, mammalian cell cytotoxicity, and antimicrobial activity". Journal of Medicinal Chemistry. 35 (25): 4745–50. doi:10.1021/jm00103a013. PMID 1469702.
- ↑ Schaumann R, Rodloff AC (January 2007). "Activities of Quinolones Against Obligately Anaerobic Bacteria" (PDF). Anti-Infective Agents in Medicinal Chemistry. 6 (1): 49–56. doi:10.2174/187152107779314179. Archived (PDF) from the original on 16 June 2010. Retrieved 6 May 2011.
- ↑ Zhanel GG, Fontaine S, Adam H, Schurek K, Mayer M, Noreddin AM, Gin AS, Rubinstein E, Hoban DJ (2006). "A Review of New Fluoroquinolones : Focus on their Use in Respiratory Tract Infections". Treat Respir Med. 5 (6): 437–65. doi:10.2165/00151829-200605060-00009. PMID 17154673. S2CID 26955572.
- ↑ sanofi-aventis U.S. LLC (September 2008). "NegGram Caplets (nalidixic acid, USP)" (PDF). Food and Drug Administration.
- ↑ Wentland MP: In memoriam: George Y. Lesher, PhD, in Hooper DC, Wolfson JS (eds): Quinolone antimicrobial agents, ed 2., Washington DC, American Society for Microbiology : XIII - XIV, 1993.
- ↑ Norris S, Mandell GL (1988). The quinolones: history and overview. San Diego: Academic Press Inc. pp. 1–22.
- 1 2 3 4 "FDA updates warnings for fluoroquinolone antibiotics". FDA. 26 July 2016.
- ↑ "Fluoroquinolone Safety Labeling Changes" (PDF). FDA. 4 April 2017. Archived from the original (PDF) on 9 May 2017.
- ↑ "Briefing Information for the November 5, 2015 Joint Meeting of the Antimicrobial Drugs Advisory Committee (AMDAC) and the Drug Safety and Risk Management Advisory Committee (DSaRM)". Food and Drug Administration. Archived from the original on 20 October 2015. Retrieved 19 October 2015.
- ↑ "FDA Briefing Document Joint Meeting of the Antimicrobial Drugs Advisory Committee and the Drug Safety and Risk Management Advisory Committee, November 5, 2015" (PDF). FDA. Archived from the original (PDF) on 17 November 2015.
- ↑ "Transcript: Joint Meeting of the Antimicrobial Drugs Advisory Committee and the Drug Safety and Risk Management Advisory Committee, November 5, 2015" (PDF). FDA. Archived from the original (PDF) on 8 February 2016.
- ↑ Burton TM (6 November 2015). "FDA Panel Seeks Tougher Antibiotic Labels". The Wall Street Journal. Retrieved 6 November 2015.
- ↑ sanofi-aventis U.S. LLC (September 2008). "NegGram® Caplets (nalidixic acid, USP)" (PDF). USA: FDA. Retrieved 6 May 2011.
- ↑ Wentland MP: In memoriam: George Y. Lesher, PhD, in Hooper DC, Wolfson JS (eds): Quinolone antimicrobial agents, ed 2., Washington DC, American Society for Microbiology : XIII – XIV, 1993.
- ↑ Ball P (2000). "Quinolone generations: natural history or natural selection?". J. Antimicrob. Chemother. 46 Suppl T1 (Supplement 3): 17–24. doi:10.1093/oxfordjournals.jac.a020889. PMID 10997595.
- ↑ Lilley SH, Malone R, King DE (May 2000). "New Classification and Update on the Quinolone Antibiotics – May 1, 2000 – American Academy of Family Physicians". American Family Physician. 61 (9): 2741–2748. Archived from the original on 6 June 2011. Retrieved 18 March 2008.
- 1 2 3 4 5 6 7 8 9 10 11 12 Oliphant CM, Green GM (February 2002). "Quinolones: a comprehensive review". American Family Physician. 65 (3): 455–64. PMID 11858629. Archived from the original on 29 September 2007. Retrieved 6 May 2011.
- 1 2 3 4 Ambrose PG, Owens Jr RC (1 March 2000). "Clinical Usefulness of Quinolones". Seminars in Respiratory and Critical Care Medicine. Archived from the original on 23 June 2011. Retrieved 6 May 2011.
- ↑ UN (2005). "Consolidated list of products – Pharmaceuticals 12th issue" (PDF). United Nations. Retrieved 6 May 2011.
- ↑ Gupta (2009). Clinical Ophthalmology: Contemporary Perspectives, 9/e. Elsevier India. pp. 112–. ISBN 978-81-312-1680-4. Retrieved 20 September 2010.
- ↑ Schmid RE (1 May 2006). "Drug Company Taking Tequin Off Market". Associated Press. Archived from the original on 25 November 2007. Retrieved 1 May 2006.
External links
- Quinolone antibiotic at Curlie
- Healthcare-associated Infections (HAIs)- Quinolones and the Clinical Laboratory CDC
- Information for Healthcare Professionals: Fluoroquinolone Antimicrobial Drugs from the U.S. Food and Drug Administration
- Fluoroquinolones Archived 17 June 2006 at the Wayback Machine "Family Practice Notebook" entry page for Fluoroquinolones
- Structure Activity Relationships "Antibacterial Agents; Structure Activity Relationships," André Bryskier MD