| X-linked hypophosphatemia | |
|---|---|
| Other names | X-linked dominant hypophosphatemic rickets, or X-linked Vitamin D-resistant rickets,[1] |
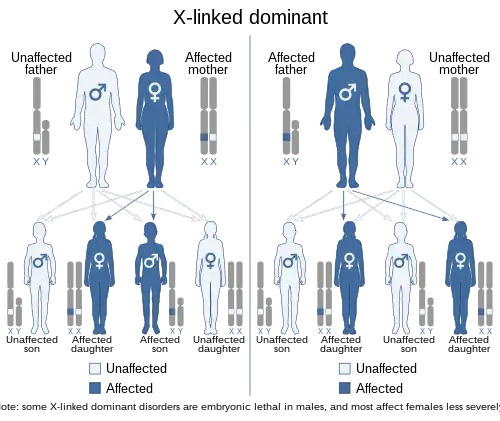 | |
| This condition is inherited in an X-linked dominant manner. | |
| Specialty | Endocrinology, pediatrics |
| Complications | osteomalacia (adults), rickets (children), fractures, enthesopathy, spinal stenosis, abnormal gait, short stature, tinnitus, hearing loss, dental complications, in rare exceptions Chiari malformation can occur. |
| Causes | A genetic mutation of the PHEX gene results in elevated FGF23 hormone. |
| Medication | phosphate, vitamin-D or burosumab |
X-linked hypophosphatemia (XLH) is an X-linked dominant form of rickets (or osteomalacia) that differs from most cases of dietary deficiency rickets in that vitamin D supplementation does not cure it. It can cause bone deformity including short stature and genu varum (bow-leggedness). It is associated with a mutation in the PHEX gene sequence (Xp.22) and subsequent inactivity of the PHEX protein.[2] PHEX mutations lead to an elevated circulating (systemic) level of the hormone FGF23 which results in renal phosphate wasting,[3] and locally in the extracellular matrix of bones and teeth an elevated level of the mineralization/calcification-inhibiting protein osteopontin.[4][5] An inactivating mutation in the PHEX gene results in an increase in systemic circulating FGF23, and a decrease in the enzymatic activity of the PHEX enzyme which normally removes (degrades) mineralization-inhibiting osteopontin protein; in XLH, the decreased PHEX enzyme activity leads to an accumulation of inhibitory osteopontin locally in bones and teeth to block mineralization which, along with renal phosphate wasting, both cause osteomalacia and odontomalacia.[6][7]
For both XLH and hypophosphatasia, inhibitor-enzyme pair relationships function to regulate mineralization in the extracellular matrix through a double-negative (inhibiting the inhibitors) activation effect in a manner described as the Stenciling Principle.[8][9] Both these underlying mechanisms (renal phosphate wasting systemically, and mineralization inhibitor accumulation locally) contribute to the pathophysiology of XLH that leads to soft bones and teeth (hypomineralization, osteomalacia/odontomalacia).[10][11][12] The prevalence of the disease is 1 in 20,000.[13]
X-linked hypophosphatemia may be lumped in with autosomal dominant hypophosphatemic rickets under general terms such as hypophosphatemic rickets. Hypophosphatemic rickets are associated with at least nine other genetic mutations.[14] Clinical management of hypophosphatemic rickets may differ depending on the specific mutations associated with an individual case, but treatments are aimed at raising phosphate levels to promote normal bone formation.[15]
Symptoms and signs
The most common symptoms of XLH affect the bones and teeth, causing pain, abnormalities, and osteoarthritis. Symptoms and signs can vary between children and adults and can include:
Children
- Rickets[16]
- Dentin defects and enamel abnormalities causing dental abscesses
- Craniostenosis[17]
- Fractures and pseudofractures
- Bone pain[18]
- Fatigue[19]
- Delayed growth
- Delayed motor development
Adults
- Osteomalacia[16]
- Dental abscesses[20]
- Limited range of movement (enthesopathy)[20] [21]
- Short stature[20]
- Fatigue[19]
- Fractures / pseudofracture[22]
- Bone pain[18] People often have bowed legs or knock knees in which they usually cannot touch both knees and ankles together at the same time.
- Craniostenosis[20]
- Osteoarthritis[23]
- Spinal stenosis[24]
- Hearing loss[20]
- Depression[25]
- Impaired innate immunity[26]
- Defective mineral tessellation (an ultrastructural mineralization deficiency)[27] [28]
Genetics
XLH affects about 1:20,000 individuals and is the most common cause of inherited phosphate wasting.[26]
It is associated with a mutation in the PHEX gene sequence, located on the human X chromosome at location Xp22.2-p22.1.[1][2][29] The PHEX protein regulates another protein called fibroblast growth factor 23 (produced from the FGF23 gene). Fibroblast growth factor 23 normally inhibits the kidneys' ability to reabsorb phosphate into the bloodstream. Gene mutations in PHEX prevent it from correctly regulating fibroblast growth factor 23. The overactivity of FGF-23 reduces vitamin D 1α-hydroxylation and phosphate reabsorption by the kidneys, leading to hypophosphatemia and the related features of ricket.[30] Also in XLH, where PHEX enzymatic activity is absent or reduced, osteopontin[31]—a mineralization-inhibiting secreted substrate protein found in the extracellular matrix of bone[32]—accumulates in bone (and teeth) to contribute to the osteomalacia (and odontomalacia) as shown in the mouse homolog (Hyp) of XLH and in XLH patients.[33][34][35]
The disorder is inherited in an X-linked dominant manner.[1][2] This means the defective gene responsible for the disorder (PHEX) is located on the X chromosome, and only one copy of the defective gene is sufficient to cause the disorder when inherited from a parent who has the disorder. Males are normally hemizygous for the X chromosome, having only one copy. As a result, X-linked dominant disorders usually show higher expressivity in males than females.
As the X chromosome is one of the sex chromosomes (the other being the Y chromosome), X-linked inheritance is determined by the sex of the parent carrying a specific gene and can often seem complex. This is because, typically, females have two copies of the X-chromosome and males have only one copy. The difference between dominant and recessive inheritance patterns also plays a role in determining the chances of a child inheriting an X-linked disorder from their parentage.
Diagnosis
The clinical laboratory evaluation of rickets begins with assessment of serum calcium, phosphate, and alkaline phosphatase levels. In hypophosphatemic rickets, calcium levels may be within or slightly below the reference range; alkaline phosphatase levels will be significantly above the reference range.Biochemically, XLH is recognized by hypophosphatemia.[36]
Carefully evaluate serum phosphate levels in the first year of life, because the concentration reference range for infants (5.0–7.5 mg/dL) is high compared with that for adults (2.7–4.5 mg/dL).
Serum parathyroid hormone levels are within the reference range or slightly elevated. calcitriol (1,25-(OH)2 vitamin D3) levels are low or within the lower reference range. Most importantly, urinary loss of phosphate is above the reference range.
The renal tubular reabsorption of phosphate (TRP) in X-linked hypophosphatemia is 60%; normal TRP exceeds 90% at the same reduced plasma phosphate concentration. The TRP is calculated with the following formula:
- 1 − [Phosphate Clearance (CPi) / Creatinine Clearance (Ccr)] × 100
Treatment
Conventional therapy consisted of medications including human growth hormone, calcitriol, and oral phosphate,[37][38] and calcitriol;[37][38] Unwanted effects of this therapy have included secondary hyperparathyroidism, nephrocalcinosis, kidney stones, and cardiovascular abnormalities.
In February 2018 the European Medicines Agency first licensed a monoclonal antibody directed against FGF23, the first drug targeting the underlying cause for this condition,[39] called burosumab.[40] It was then licensed by the US Food and Drug Administration in June 2018[41]
The leg deformity can be treated with Ilizarov frames and CAOS.[42] In the event of severe bowing, an osteotomy can be performed to correct the leg shape.[42]
Society and culture
International XLH Alliance – an alliance of international patient groups for individuals affected by XLH and related disorders.
Jennyfer Marques Parinos is a Paralympic bronze medalist from Brazil who has XLH. She competes under a class 9 disability.
See also
References
- 1 2 3 Online Mendelian Inheritance in Man (OMIM): 307800"HYPOPHOSPHATEMIC RICKETS, X-LINKED DOMINANT; XLHR". 23 June 2023.
- 1 2 3 Saito, T.; Nishii, Y.; Yasuda, T.; Ito, N.; Suzuki, H.; Igarashi, T.; Fukumoto, S.; Fujita, T. (Oct 2009). "Familial hypophosphatemic rickets caused by a large deletion in PHEX gene". European Journal of Endocrinology. 161 (4): 647–651. doi:10.1530/EJE-09-0261. PMID 19581284.
- ↑ Carpenter, TO; Feingold, KR; Anawalt, B; Boyce, A; Chrousos, G; de Herder, WW; Dhatariya, K; Dungan, K; Hershman, JM; Hofland, J; Kalra, S; Kaltsas, G; Koch, C; Kopp, P; Korbonits, M; Kovacs, CS; Kuohung, W; Laferrère, B; Levy, M; McGee, EA; McLachlan, R; Morley, JE; New, M; Purnell, J; Sahay, R; Singer, F; Sperling, MA; Stratakis, CA; Trence, DL; Wilson, DP (2000). "Primary Disorders of Phosphate Metabolism". PMID 25905395.
{{cite journal}}: Cite journal requires|journal=(help) - ↑ Barros, NM; Hoac, B; Neves, RL; Addison, WN; Assis, DM; Murshed, M; Carmona, AK; McKee, MD (March 2013). "Proteolytic processing of osteopontin by PHEX and accumulation of osteopontin fragments in Hyp mouse bone, the murine model of X-linked hypophosphatemia". Journal of Bone and Mineral Research. 28 (3): 688–99. doi:10.1002/jbmr.1766. PMID 22991293. S2CID 20840491.
- ↑ Boukpessi, T; Hoac, B; Coyac, BR; Leger, T; Garcia, C; Wicart, P; Whyte, MP; Glorieux, FH; Linglart, A; Chaussain, C; McKee, MD (February 2017). "Osteopontin and the dento-osseous pathobiology of X-linked hypophosphatemia". Bone. 95: 151–161. doi:10.1016/j.bone.2016.11.019. PMID 27884786.
- ↑ Boukpessi, T.; Hoac, B.; Coyac, B. R.; Leger, T.; Garcia, C.; Wicart, P.; Whyte, M. P.; Glorieux, F. H.; Linglart, A.; Chaussain, C.; McKee, M. D. (2017). "Osteopontin and the dento-osseous pathobiology of X-linked hypophosphatemia". Bone. 95: 151–161. doi:10.1016/j.bone.2016.11.019. PMID 27884786.
- ↑ Barros, N. M.; Hoac, B.; Neves, R. L.; Addison, W. N.; Assis, D. M.; Murshed, M.; Carmona, A. K.; McKee, M. D. (2013). "Proteolytic processing of osteopontin by PHEX and accumulation of osteopontin fragments in Hyp mouse bone, the murine model of X-linked hypophosphatemia". Journal of Bone and Mineral Research. 28 (3): 688–699. doi:10.1002/jbmr.1766. PMID 22991293. S2CID 20840491.
- ↑ Reznikov, N.; Hoac, B.; Buss, D. J.; Addison, W. N.; Barros NMT; McKee, M. D. (2020). "Biological stenciling of mineralization in the skeleton: Local enzymatic removal of inhibitors in the extracellular matrix". Bone. 138: 115447. doi:10.1016/j.bone.2020.115447. PMID 32454257. S2CID 218909350.
- ↑ McKee, M. D.; Buss, D. J.; Reznikov, N. (2022). "Mineral tessellation in bone and the Stenciling Principle for extracellular matrix mineralization". Journal of Structural Biology. 214 (1): 107823. doi:10.1016/j.jsb.2021.107823. PMID 34915130. S2CID 245187449.
- ↑ McKee, MD; Buss, DJ; Reznikov, N (13 December 2021). "Mineral tessellation in bone and the stenciling principle for extracellular matrix mineralization". Journal of Structural Biology. 214 (1): 107823. doi:10.1016/j.jsb.2021.107823. PMID 34915130. S2CID 245187449.
- ↑ McKee, MD; Hoac, B; Addison, WN; Barros, NM; Millán, JL; Chaussain, C (October 2013). "Extracellular matrix mineralization in periodontal tissues: Noncollagenous matrix proteins, enzymes, and relationship to hypophosphatasia and X-linked hypophosphatemia". Periodontology 2000. 63 (1): 102–22. doi:10.1111/prd.12029. PMC 3766584. PMID 23931057.
- ↑ Buss, DJ; Reznikov, N; McKee, MD (1 November 2020). "Crossfibrillar mineral tessellation in normal and Hyp mouse bone as revealed by 3D FIB-SEM microscopy". Journal of Structural Biology. 212 (2): 107603. doi:10.1016/j.jsb.2020.107603. PMID 32805412. S2CID 221164596.
- ↑ Carpenter TO (Apr 1997). "New perspectives on the biology and treatment of X-linked hypophosphatemic rickets". Pediatr. Clin. North Am. 44 (2): 443–466. doi:10.1016/S0031-3955(05)70485-5. PMID 9130929.
- ↑ Online Mendelian Inheritance in Man (OMIM): 193100
- ↑ "Hypophosphatemic rickets". Genetic and Rare Diseases Information Center. National Institutes of Health. Archived from the original on 12 June 2012. Retrieved 10 October 2012.
- 1 2 "Osteomalacia and Rickets". The Lecturio Medical Concept Library. Retrieved 24 August 2021.
- ↑ Silva S, Jeanty P (1999-06-07). "Cloverleaf skull or kleeblattschadel". TheFetus.net. MacroMedia. Archived from the original on 2007-01-07. Retrieved 2007-02-03.
- 1 2 Luger, N. Mach, D. Sevcik, M. Mantyh, P. (2005). Bone cancer pain: From mechanism to model to therapy. Journal of Pain and Symptom Management. 29(5): 32-46.
- 1 2 "Fatigue". MedlinePlus. Retrieved April 30, 2020.
- 1 2 3 4 5 Linglart, A.; Biosse-Duplan, M.; Briot, K.; Chaussain, C.; Esterle, L.; Guillaume-Czitrom, S.; Kamenicky, P.; Nevoux, J.; Prié, D.; Rothenbuhler, A.; Wicart, P.; Harvengt, P. (2014). "Therapeutic management of hypophosphatemic rickets from infancy to adulthood". Endocrine Connections. 3 (1): R13–R30. doi:10.1530/EC-13-0103. PMC 3959730. PMID 24550322.
- ↑ Buss, Daniel J.; Rechav, Katya; Reznikov, Natalie; McKee, Marc D. (September 2023). "Mineral tessellation in mouse enthesis fibrocartilage, Achilles tendon, and Hyp calcifying enthesopathy: A shared 3D mineralization pattern". Bone. 174: 116818. doi:10.1016/j.bone.2023.116818. ISSN 8756-3282. PMID 37295663. S2CID 259131061.
- ↑ "Overview of Bone Fractures". The Lecturio Medical Concept Library. Retrieved 24 August 2021.
- ↑ "Osteoarthritis". The Lecturio Medical Concept Library. Retrieved 24 August 2021.
- ↑ Skrinar, A.; Dvorak-Ewell, M.; Evins, A.; MacIca, C.; Linglart, A.; Imel, E. A.; Theodore-Oklota, C.; San Martin, J. (2019). "The Lifelong Impact of X-Linked Hypophosphatemia: Results From a Burden of Disease Survey". Journal of the Endocrine Society. 3 (7): 1321–1334. doi:10.1210/js.2018-00365. PMC 6595532. PMID 31259293.
- ↑ Hawley, S.; Shaw, N. J.; Delmestri, A.; Prieto-Alhambra, D.; Cooper, C.; Pinedo-Villanueva, R.; Javaid, M. K. (2020). "Higher prevalence of non-skeletal comorbidity related to X-linked hypophosphataemia: a UK parallel cohort study using CPRD". Rheumatology. 60 (9): 4055–4062. doi:10.1093/rheumatology/keaa859. PMID 33331900.
- 1 2 Beck-Nielsen, Signe Sparre; Mughal, Zulf; Haffner, Dieter; Nilsson, Ola; Levtchenko, Elena; Ariceta, Gema; de Lucas Collantes, Carmen; Schnabel, Dirk; Jandhyala, Ravi; Mäkitie, Outi (2019-02-26). "FGF23 and its role in X-linked hypophosphatemia-related morbidity". Orphanet Journal of Rare Diseases. 14 (1): 58. doi:10.1186/s13023-019-1014-8. ISSN 1750-1172. PMC 6390548. PMID 30808384.
- ↑ Buss, Daniel J.; Reznikov, Natalie; McKee, Marc D. (November 2020). "Crossfibrillar mineral tessellation in normal and Hyp mouse bone as revealed by 3D FIB-SEM microscopy". Journal of Structural Biology. 212 (2): 107603. doi:10.1016/j.jsb.2020.107603. ISSN 1047-8477. PMID 32805412. S2CID 221164596.
- ↑ Buss, Daniel J.; Rechav, Katya; Reznikov, Natalie; McKee, Marc D. (September 2023). "Mineral tessellation in mouse enthesis fibrocartilage, Achilles tendon, and Hyp calcifying enthesopathy: A shared 3D mineralization pattern". Bone. 174: 116818. doi:10.1016/j.bone.2023.116818. ISSN 8756-3282. PMID 37295663. S2CID 259131061.
- ↑ 300550"PHOSPHATE-REGULATING ENDOPEPTIDASE HOMOLOG, X-LINKED; PHEX". 18 April 2011.
{{cite web}}: Missing or empty|url=(help) - ↑ Perwad, Farzana; Zhang, Martin Y. H.; Tenenhouse, Harriet S.; Portale, Anthony A. (2007-11-01). "Fibroblast growth factor 23 impairs phosphorus and vitamin D metabolism in vivo and suppresses 25-hydroxyvitamin D-1alpha-hydroxylase expression in vitro". American Journal of Physiology. Renal Physiology. 293 (5): F1577–1583. doi:10.1152/ajprenal.00463.2006. ISSN 1931-857X. PMID 17699549. S2CID 20559055.
- ↑ Sodek, J; et al. (2000). "Osteopontin". Critical Reviews in Oral Biology and Medicine. 11 (3): 279–303. doi:10.1177/10454411000110030101. PMID 11021631.
- ↑ McKee, MD; et al. (2005). "Hierarchies of extracellular matrix and mineral organization in bone of the craniofacial complex and skeleton". Cells Tissues Organs. 181 (3–4): 176–188. doi:10.1159/000091379. PMID 16612083. S2CID 40705942.
- ↑ McKee, MD; Hoac, B; Addison, WN; Barros, NM; Millán, JL; Chaussain, C (October 2013). "Extracellular matrix mineralization in periodontal tissues: Noncollagenous matrix proteins, enzymes, and relationship to hypophosphatasia and X-linked hypophosphatemia". Periodontology 2000. 63 (1): 102–22. doi:10.1111/prd.12029. PMC 3766584. PMID 23931057.
- ↑ Boukpessi, T; Hoac, B; Coyac, BR; Leger, T; Garcia, C; Wicart, P; Whyte, MP; Glorieux, FH; Linglart, A; Chaussain, C; McKee, MD (21 November 2016). "Osteopontin and the dento-osseous pathobiology of X-linked hypophosphatemia". Bone. 95: 151–161. doi:10.1016/j.bone.2016.11.019. PMID 27884786.
- ↑ Barros, NMT; et al. (2013). "Proteolytic processing of osteopontin by PHEX and accumulation of osteopontin fragments in Hyp mouse bone, the murine model of X-linked hypophosphatemia". Journal of Bone and Mineral Research. 28 (3): 688–699. doi:10.1002/jbmr.1766. PMID 22991293.
- ↑ Haffner, Dieter; Emma, Francesco; Eastwood, Deborah M.; Duplan, Martin Biosse; Bacchetta, Justine; Schnabel, Dirk; Wicart, Philippe; Bockenhauer, Detlef; Santos, Fernando; Levtchenko, Elena; Harvengt, Pol; Kirchhoff, Martha; Di Rocco, Federico; Chaussain, Catherine; Brandi, Maria Louisa (July 2019). "Clinical practice recommendations for the diagnosis and management of X-linked hypophosphataemia". Nature Reviews Nephrology. 15 (7): 435–455. doi:10.1038/s41581-019-0152-5. ISSN 1759-507X. PMC 7136170. PMID 31068690.
- 1 2 Imel, E. A.; DiMeglio, L. A.; Hui, S. L.; Carpenter, T. O.; Econs, M. J. (15 February 2010). "Treatment of X-Linked Hypophosphatemia with Calcitriol and Phosphate Increases Circulating Fibroblast Growth Factor 23 Concentrations". Journal of Clinical Endocrinology & Metabolism. 95 (4): 1846–1850. doi:10.1210/jc.2009-1671. PMC 2853995. PMID 20157195.
- 1 2 Glorieux, F. H.; Marie, P. J.; Pettifor, J. M.; Delvin, E. E. (30 October 1980). "Bone response to phosphate salts, ergocalciferol, and calcitriol in hypophosphatemic vitamin D-resistant rickets". The New England Journal of Medicine. 303 (18): 1023–1031. doi:10.1056/NEJM198010303031802. PMID 6252463.
- ↑ Carpenter, TO; Whyte MP; Imel EA; Boot AM; Högler W; Linglart A; Padidela R; Van't Hoff W; Mao M; Chen CY; Skrinar A; Kakkis E; San Martin J; Portale AA (24 May 2018). "Burosumab Therapy in Children with X-Linked Hypophosphatemia". The New England Journal of Medicine (Submitted manuscript). 378 (21): 1987–1998. doi:10.1056/NEJMoa1714641. hdl:1805/18603. PMID 29791829. S2CID 44135503.
- ↑ "EMA authorisation details". 17 September 2018.
- ↑ "FDA press release".
- 1 2 "X-linked hypophosphatemia | Genetic and Rare Diseases Information Center (GARD) – an NCATS Program". rarediseases.info.nih.gov. Retrieved 2018-10-21.