| SOFA score | |
|---|---|
 A patient's SOFA score assessment | |
| Purpose | determine rate of organ failure |
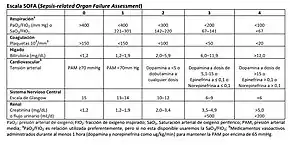
The sequential organ failure assessment score (SOFA score), previously known as the sepsis-related organ failure assessment score,[1] is used to track a person's status during the stay in an intensive care unit (ICU) to determine the extent of a person's organ function or rate of failure.[2][3][4][5][6] The score is based on six different scores, one each for the respiratory, cardiovascular, hepatic, coagulation, renal and neurological systems.
The score tables below only describe points-giving conditions. In cases where the physiological parameters do not match any row, zero points are given. In cases where the physiological parameters match more than one row, the row with most points is picked.
The quick SOFA score (qSOFA) assists health care providers in estimating the risk of morbidity and mortality due to sepsis.[7]
Medical use
The SOFA scoring system is useful in predicting the clinical outcomes of critically ill patients.[8] According to an observational study at an Intensive Care Unit (ICU) in Belgium, the mortality rate is at least 50% when the score is increased, regardless of initial score, in the first 96 hours of admission, 27% to 35% if the score remains unchanged, and less than 27% if the score is reduced.[9] Score ranges from 0 (best) to 24 (worst) points.[10]
| Central nervous system | Cardiovascular system | Respiratory system | Coagulation | Liver | Renal function | |
|---|---|---|---|---|---|---|
| Score | Glasgow coma scale | Mean arterial pressure OR administration of vasopressors required | PaO2/FiO2 [mmHg (kPa)] | Platelets (×103/μl) | Bilirubin (mg/dl) [μmol/L] | Creatinine (mg/dl) [μmol/L] (or urine output) |
| +0 | 15 | MAP ≥ 70 mmHg | ≥ 400 (53.3) | ≥ 150 | < 1.2 [< 20] | < 1.2 [< 110] |
| +1 | 13–14 | MAP < 70 mmHg | < 400 (53.3) | < 150 | 1.2–1.9 [20-32] | 1.2–1.9 [110-170] |
| +2 | 10–12 | dopamine ≤ 5 μg/kg/min or dobutamine (any dose) | < 300 (40) | < 100 | 2.0–5.9 [33-101] | 2.0–3.4 [171-299] |
| +3 | 6–9 | dopamine > 5 μg/kg/min OR epinephrine ≤ 0.1 μg/kg/min OR norepinephrine ≤ 0.1 μg/kg/min | < 200 (26.7) and mechanically ventilated including CPAP | < 50 | 6.0–11.9 [102-204] | 3.5–4.9 [300-440] (or < 500 ml/day) |
| +4 | < 6 | dopamine > 15 μg/kg/min OR epinephrine > 0.1 μg/kg/min OR norepinephrine > 0.1 μg/kg/min | < 100 (13.3) and mechanically ventilated including CPAP | < 20 | > 12.0 [> 204] | > 5.0 [> 440] (or < 200 ml/day) |
Quick SOFA score
The Quick SOFA Score (quickSOFA or qSOFA) was introduced by the Sepsis-3 group in February 2016 as a simplified version of the SOFA Score as an initial way to identify patients at high risk for poor outcome with an infection.[11] The SIRS Criteria definitions of sepsis are being replaced as they were found to possess too many limitations; the "current use of 2 or more SIRS criteria to identify sepsis was unanimously considered by the task force to be unhelpful." The qSOFA simplifies the SOFA score drastically by only including its 3 clinical criteria and by including "any altered mentation" instead of requiring a GCS <15. qSOFA can easily and quickly be repeated serially on patients.
| Assessment | qSOFA score |
|---|---|
| Low blood pressure (SBP ≤ 100 mmHg) | 1 |
| High respiratory rate (≥ 22 breaths/min) | 1 |
| Altered mentation (GCS ≤ 14) | 1 |
The score ranges from 0 to 3 points. The presence of 2 or more qSOFA points near the onset of infection was associated with a greater risk of death or prolonged intensive care unit stay. These are outcomes that are more common in infected patients who may be septic than those with uncomplicated infection. Based upon these findings, the Third International Consensus Definitions for Sepsis recommends qSOFA as a simple prompt to identify infected patients outside the ICU who are likely to be septic.[12]
qSOFA has also been found to be poorly sensitive though decently specific for the risk of death with SIRS possibly better for screening.[13]
qSOFA utility
The qSOFA was designed to be used in non-ICU settings, where the healthcare provider might not have access to all the information used in the SOFA score. Settings include the emergency department or other healthcare settings where patients are initially assessed. The three criteria used (systolic blood pressure, respiratory rate, and GCS) can be quickly gathered in the emergency department, to risk stratify patients and provide potentially ill patients with quick interventions. This scoring system is used to identify potential patients with sepsis.[14]
In 2019, the surviving sepsis campaign detailed a bundle of medical interventions to be done within the first hour of presentation on septic patients to reduce mortality, so quick identification of these patients with the qSOFA score is important to treat quickly. This group of interventions is the one hour bundle and includes:[15]
- Measure lactate level
- Draw blood culture before starting antibiotics
- Start broad spectrum antibiotics
- Rapidly give crystalloid if hypotensive or lactate greater than or equal to 4 mmol/L
- Give vasopressors if still hypotensive after crystalloid administration
One study found the one hour bundle to have no significant improvement in in-hospital mortality over patients given the 3 or 6 hour bundles that have been previously recommended by the surviving sepsis campaign.[16]
See also
References
- ↑ Singer, Mervyn; et al. (23 February 2016). "The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3)". JAMA. 315 (8): 801–10. doi:10.1001/jama.2016.0287. PMC 4968574. PMID 26903338.
- ↑ Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, Reinhart CK, Suter PM, Thijs LG (Jul 1996). "The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine". Intensive Care Med. 22 (7): 707–10. doi:10.1007/bf01709751. PMID 8844239. S2CID 40396839.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ↑ Vincent JL, de Mendonça A, Cantraine F, Moreno R, Takala J, Suter PM, Sprung CL, Colardyn F, Blecher S (Nov 1998). "Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working group on "sepsis-related problems" of the European Society of Intensive Care Medicine". Crit Care Med. 26 (11): 1793–800. doi:10.1097/00003246-199811000-00016. PMID 9824069. S2CID 28070236.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ↑ Moreno R, Vincent JL, Matos R, Mendonça A, Cantraine F, Thijs L, Takala J, Sprung C, Antonelli M, Bruining H, Willatts S (Jul 1999). "The use of maximum SOFA score to quantify organ dysfunction/failure in intensive care. Results of a prospective, multicentre study. Working Group on Sepsis related Problems of the ESICM". Intensive Care Med. 25 (7): 686–96. doi:10.1007/s001340050931. PMID 10470572. S2CID 34510892.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ↑ de Mendonça A, Vincent JL, Suter PM, Moreno R, Dearden NM, Antonelli M, Takala J, Sprung C, Cantraine F (Jul 2000). "Acute renal failure in the ICU: risk factors and outcome evaluated by the SOFA score". Intensive Care Med. 26 (7): 915–21. doi:10.1007/s001340051281. PMID 10990106. S2CID 24304874.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ↑ Ferreira FL, Bota DP, Bross A, Mélot C, Vincent JL (Oct 2001). "Serial evaluation of the SOFA score to predict outcome in critically ill patients". JAMA. 286 (14): 1754–8. doi:10.1001/jama.286.14.1754. PMID 11594901.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ↑ "National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2013". www.hcup-us.ahrq.gov. Rockville, MD: Agency for Healthcare Research and Quality. Retrieved 2017-01-07.
- ↑ Vincent, JL; de Mendonca, A; Cantraine, F; Monero, R; Takala, J; Suter, PM; Sprung, CL (November 1998). "Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working group on "sepsis-related problems" of the European Society of Intensive Care Medicine". Critical Care Medicine. 26 (11): 1793–800. doi:10.1097/00003246-199811000-00016. PMID 9824069. S2CID 28070236.
- ↑ Ferreira, FL; Bota, DP; Bross, A; Melot, C; Vincent, JL (10 October 2001). "Serial evaluation of the SOFA score to predict outcome in critically ill patients". Journal of the American Medical Association. 286 (14): 1754–1758. doi:10.1001/jama.286.14.1754. PMID 11594901.
- ↑ Raith, Eamon P.; Udy, Andrew A.; Bailey, Michael; McGloughlin, Steven; MacIsaac, Christopher; Bellomo, Rinaldo; Pilcher, David V.; for the Australian and New Zealand Intensive Care Society (ANZICS) Centre for Outcomes and Resource Evaluation (CORE) (2017-01-17). "Prognostic Accuracy of the SOFA Score, SIRS Criteria, and qSOFA Score for In-Hospital Mortality Among Adults With Suspected Infection Admitted to the Intensive Care Unit". JAMA. 317 (3): 290–300. doi:10.1001/jama.2016.20328. ISSN 0098-7484. PMID 28114553. S2CID 205078408.
- ↑ Angus, Derek C.; Seymour, Christopher W.; Coopersmith, Craig M.; Deutschman, Clifford S.; Klompas, Michael; Levy, Mitchell M.; Martin, Gregory S.; Osborn, Tiffany M.; Rhee, Chanu (2016). "A Framework for the Development and Interpretation of Different Sepsis Definitions and Clinical Criteria". Critical Care Medicine. 44 (3): e113–e121. doi:10.1097/ccm.0000000000001730. PMC 4765912. PMID 26901559.
- ↑ "qSOFA :: What is qSOFA?". www.qsofa.org. Retrieved 2016-05-29.
- ↑ Fernando, Shannon M.; Tran, Alexandre; Taljaard, Monica; Cheng, Wei; Rochwerg, Bram; Seely, Andrew J.E.; Perry, Jeffrey J. (6 February 2018). "Prognostic Accuracy of the Quick Sequential Organ Failure Assessment for Mortality in Patients With Suspected Infection". Annals of Internal Medicine. 168 (4): 266–275. doi:10.7326/M17-2820. PMID 29404582. S2CID 3441582.
- ↑ Norse, Ashley; Guirgis, Faheem. "Updates and Controversies in the Early Management of Sepsis and Septic Shock | EB Medicine". www.ebmedicine.net. EBMedicine.
- ↑ "Hour-1 Bundle" (PDF). Surviving Sepsis Campaign. Society of Critical Care Medicine and the European Society of Intensive Care Medicine.
- ↑ Ko, BS; Choi, SH; Shin, TG; Kim, K; Jo, YH; Ryoo, SM; Park, YS; Kwon, WY; Choi, HS; Chung, SP; Suh, GJ; Kang, H; Lim, TH; Son, D; Kim, WY (2 February 2021). "Impact of 1-Hour Bundle Achievement in Septic Shock". Journal of Clinical Medicine. 10 (3): 527. doi:10.3390/jcm10030527. PMC 7867161. PMID 33540513.
External links
- Janssens U; et al. (2001). "Value of SOFA (Sequential Organ Failure Assessment) score and total maximum SOFA score in 812 patients with acute cardiovascular disorders". Crit Care. 5 (S1): P225. doi:10.1186/cc1292. PMC 3333412.