| Triangle of auscultation | |
|---|---|
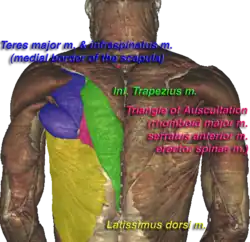 Triangle of auscultation (shown in pink) of the Visible Human Male | |
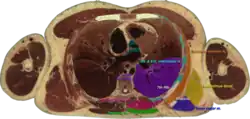 Cross section #1428 of the Visible Human Male showing the structures of the triangle of auscultation | |
| Details | |
| Identifiers | |
| Latin | trigonum auscultationis |
| TA98 | A01.2.05.006 |
| TA2 | 267 |
| FMA | 75022 |
| Anatomical terminology | |
The triangle of auscultation is a relative thinning of the musculature of the back, situated along the medial border of the scapula which allows for improved listening to the lungs.
Boundaries
It has the following boundaries:
- medially, by the inferior portion of the trapezius
- inferiorly, by the latissimus dorsi
- laterally, by the medial border of the scapula
The superficial floor of the triangle is formed by the lateral portion of the erector spinae muscles. Deep to these muscles are the osseous portions of the 6th and 7th ribs and the internal and external intercostal muscles.
Clinical significance
The triangle of auscultation is useful for assessment using a pulmonary auscultation and thoracic procedures.[1] Due to the relative thinning of the musculature of the back in the triangle, the posterior thoracic wall is closer to the skin surface, making respiratory sounds audible more clearly with a stethoscope. On the left side, the cardiac orifice of the stomach lies deep to the triangle. In days before X-rays were discovered, the sound of swallowed liquids were auscultated over this triangle to confirm an oesophageal tumour. To better expose the floor of the triangle up of the posterior thoracic wall in the 6th and 7th intercostal space, a patient is asked to fold their arms across their chest, laterally rotating the scapulae, while bending forward at the trunk, somewhat resembling the fetal position.
The triangle of auscultation can be used as a surgical approach path.[2][3] It can also be used for applying a nerve block known as the rhomboid intercostal block, which can be used to relieve pain after rib fractures, and a thoracotomy. This nerve block is usually achieved by injection of the local anesthetic agent into the fascial plane between the rhomboid upper intercostal muscle and the rhombic muscles.[4][5][6]
References
![]() This article incorporates text in the public domain from page 434 of the 20th edition of Gray's Anatomy (1918)
This article incorporates text in the public domain from page 434 of the 20th edition of Gray's Anatomy (1918)
- ↑ Malik, Nazish; Tedder, Brandon L.; Zemaitis, Michael R. (2020), "Anatomy, Thorax, Triangle of Auscultation", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 30969656, retrieved 2020-11-02
- ↑ Horowitz, Michael D.; Ancalmo, Nelson; Ochsner, John L. (May 1989). "Thoracotomy through the auscultatory triangle". The Annals of Thoracic Surgery. 47 (5): 782–783. doi:10.1016/0003-4975(89)90148-3. ISSN 0003-4975. PMID 2730202.
- ↑ Gandy, Kimberly L.; Hoffman, George M.; Vanderwal, Patrick; Tweddell, James S. (2010-01-01), Anderson, Robert H.; Baker, Edward J.; Penny, Daniel J.; Redington, Andrew N. (eds.), "CHAPTER 13 - Surgical Techniques", Paediatric Cardiology (Third Edition), Philadelphia: Churchill Livingstone, pp. 219–237, doi:10.1016/b978-0-7020-3064-2.00013-8, ISBN 978-0-7020-3064-2, retrieved 2020-11-02
- ↑ Yayik, Ahmet Murat; Aydin, Muhammed Enes; Tekin, Erdal; Ulas, Ali Bilal; Ahiskalioglu, Ali (December 2012). "An alternative plane block for multiple rib fractures: Rhomboid Intercostal and Sub-Serratus block (RISS)". The American Journal of Emergency Medicine. 37 (12): 2263.e5–2263.e7. doi:10.1016/j.ajem.2019.158429. ISSN 0735-6757. PMID 31526541. S2CID 202673902.
- ↑ Ökmen, K (1 April 2019). "Efficacy of rhomboid intercostal block for analgesia after thoracotomy". The Korean Journal of Pain. 32 (2): 129–132. doi:10.3344/kjp.2019.32.2.129. PMC 6549589. PMID 31091512.
- ↑ Chen, R; Su, S; Shu, H (16 March 2022). "Efficacy and safety of rhomboid intercostal block for analgesia in breast surgery and thoracoscopic surgery: a meta-analysis". BMC Anesthesiology. 22 (1): 71. doi:10.1186/s12871-022-01599-4. PMC 8925179. PMID 35296252.
External links
- Anatomy photo:01:02-0103 at the SUNY Downstate Medical Center
- Overview and diagram at ithaca.edu