膀胱輸尿管返流
膀胱輸尿管返流()是尿從膀胱到输尿管或腎的異常地反向性地流動。尿液的正常運行是從腎臟進經由輸尿管到膀胱。
| 膀胱輸尿管返流 () | |
|---|---|
 | |
| 类型 | ureteral disease[*]、疾病 |
| 分类和外部资源 | |
| 醫學專科 | 泌尿外科 |
| ICD-10 | N13.7 |
| ICD-9-CM | 593.7 |
| OMIM | |
| DiseasesDB | 13835 |
| MedlinePlus | 000459 |
| eMedicine | ped/2750 |
| MeSH | D014718 |
| Orphanet | 289365 |
症狀和病徵
出生前胎兒的膀胱輸尿管反流的症狀可能以"產前腎積水"、输尿管異常擴大、或泌尿道感染或則"急性腎盂腎炎(pyelonephritis)"之症狀出現。
新生兒可能昏昏欲睡(Lethargy)乏力地成長,而嬰幼兒及年幼的孩子呈現的典型症狀為发热、尿痛(dysuria)、多尿症、惡臭尿(malodorous urine)及消化作用(GIT)等症狀,但只有當尿路感染才會呈現VUR的初期症狀。
病因
健康的個體上輸尿管會傾斜地進入膀胱及在粘膜下運行一段距離。因此、除了在輸尿管的肌肉附著外,而這有助於在後側安全地支住它們。所有這些特點都產生"閥門似的效果"、在尿液的存儲及排尿期間能閉塞住輸尿管的開口。在人與VUR,這種機制發生故障時,與尿所得逆行流。
哈爾迪卡爾氏綜合徵(Hardikar syndrome)具有膀胱輸尿管返流、腎積水、唇顎裂、腸梗阻(Bowel obstruction)及其它的症狀。[1]
原發性VUR
Insufficient submucosal length of the ureter relative to its diameter causes inadequacy of the valvular mechanism. This is precipitated by a congenital defect/lack of longitudinal muscle of the intravesical ureter resulting in an ureterovesicular junction (UVJ) anomaly.
繼發性VUR
In this category the valvular mechanism is intact and healthy to start with but becomes overwhelmed by raised vesicular pressures associated with obstruction, which distorts the ureterovesical junction. The obstructions may be anatomical or functional. Secondary VUR can be further divided into anatomical and functional groups as follows:
解剖性:後尿道瓣膜;尿道、或"尿道外口狹窄"(meatal stenosis)。
可能時這些病因會在外科手術時進行處理。
功能性:膀胱不穩定、神經源性膀胱及非神經源性性膀胱。
膀胱輸尿管返流的國際分類
- 第I級 - 回流到非擴張的輸尿管。
- 第II級 – 無擴張的回流入腎盂腎盞。
- 第III級 – mild/moderate dilatation of the ureter, renal pelvis and calyces with minimal blunting of the fornices
- 第IV級 – dilation of the renal pelvis and calyces with moderate ureteral tortuosity
- 第V級 – gross dilatation of the ureter, pelvis and calyces; ureteral tortuosity; loss of papillary impressions
The younger the age of the patient and the lower the grade at presentation the higher the chance of spontaneous resolution. Most (approx. 85%) of grade I & II cases of VUR will resolve spontaneously. Approximately 50% of grade III cases and a lower percentage of higher grades will also resolve spontaneously.
診斷
以下的過程可用於診斷VUR:
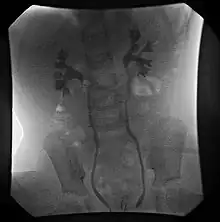
- 核膀胱造影術(cystogram)(RNC)。
- 透視(Fluoroscopic)排泄性膀胱尿道造影照片(voiding cystourethrogram)(VCUG)
- 超聲膀胱造影(Ultrasonic cystography)
- 腹部超聲波診斷。
An abdominal ultrasound might suggest the presence of VUR if ureteral dilatation is present; however, in many circumstances of VUR of low to moderate severity, the sonogram may be completely normal, thus providing insufficient utility as a single diagnostic test in the evaluation of children suspected of having VUR, such as those presenting with prenatal hydronephrosis or urinary tract infection (UTI).
VCUG is the method of choice for grading and initial workup, while RNC is preferred for subsequent evaluations as there is less exposure to radiation. A high index of suspicion should be attached to any case a where a child presents with a urinary tract infection, and anatomical causes should be excluded. A VCUG and abdominal ultrasound should be performed in these cases
Early diagnosis in children is crucial as studies have shown that the children with VUR who present with a UTI and associated acute pyelonephritis are more likely to develop permanent renal cortical scarring than those children without VUR, with an odds ratio of 2.8.[3] Thus VUR not only increases the frequency of UTI's, but also the risk of damage to upper urinary structures.
治療
The goal of treatment is to minimize infections, as it is infections that cause renal scarring and not the vesicoureteral reflux.[4] Minimizing infections is primarily done by prophylactic antibiotics in newborns and infants who are not potty trained. However in children who are older, physicians and parents should focus on bowel and bladder management. Children who hold their bladder or who are constipated have a greater number of infections than children who void on a regular schedule. When medical management fails to prevent recurrent urinary tract infections, or if the kidneys show progressive renal scaring then surgical interventions may be necessary. Medical management is recommended in children with Grade I-III VUR as most cases will resolve spontaneously. A trial of medical treatment is indicated in patients with Grade IV VUR especially in younger patients or those with unilateral disease. Of the patients with Grade V VUR only infants are trialled on a medical approach before surgery is indicated, in older patients surgery is the only option.-->
內鏡下注射
Endoscopic injection involves applying a gel around the ureteral opening to create a valve function and stop urine from flowing back up the ureter. The gel consists of two types of sugar-based molecules called dextranomer and hyaluronic acid. Trade names for this combination include Deflux and Zuidex. Both constituents are well-known from previous uses in medicine. They are also biocompatible, which means that they do not cause significant reactions within the body. In fact, hyaluronic acid is produced and found naturally within the body.
醫療
Medical treatment entails low dose antibiotic prophylaxis until resolution of VUR occurs. Antibiotics are administered nightly at half the normal therapeutic dose. The specific antibiotics used differ with the age of the patient and include:
經過2個月以下的抗生素都適合:
Urine cultures are performed 3 monthly to exclude breakthrough infection. Annual radiological investigations are likewise indicated. Good perineal hygiene, and timed and double voiding are also important aspects of medical treatment. Bladder dysfunction is treated with the administration of anticholinergics.
手術治療
A surgical approach is necessary in cases where a breakthrough infection results despite prophylaxis, or there is non-compliance with the prophylaxis. Similarly if the VUR is severe (Grade IV & V), there are pyelonephritic changes or congenital abnormalities. Other reasons necessitating surgical intervention are failure of renal growth, formation of new scars, renal deterioration and VUR in girls approaching puberty.
There are three types of surgical procedure available for the treatment of VUR: endoscopic (STING/HIT procedures); laparoscopic; and open procedures (Cohen procedure, Leadbetter-Politano procedure).
流行病學
據估計、VUR存在於人口超過10%以上。
以後發展
美國泌尿協會(American Urological Association)建議持續監測膀胱輸尿管返流的患兒、直至異常解決或不再有臨床顯著病徵。
註釋
- . [2015-01-01]. (原始内容存档于2021-03-24).
- Institute of Urology & Nephrology, London, UK, The cellular basis of bladder instability (页面存档备份,存于) UJUS 2009, Retrieved 4-20-2010
- Craig A. Peters; Steven J. Skoog; Billy S. Arant; Hillary L. Copp; Jack S. Elder; R. Guy Hudson; Antoine E. Khoury; Armando J. Lorenzo; Hans G. Pohl; Ellen Shapiro; Warren T. Snodgrass; Mireya Diaz. . The Journal of Urology. September 2010, 184 (3): 1134–44. PMID 20650499. doi:10.1016/j.juro.2010.05.065.
- Tekgül, S; Riedmiller, H; Hoebeke, P; Kočvara, R; Nijman, RJ; Radmayr, C; Stein, R; Dogan, HS; European Association of, Urology. . European Urology. September 2012, 62 (3): 534–42. PMID 22698573. doi:10.1016/j.eururo.2012.05.059.