| Cuboid syndrome | |
|---|---|
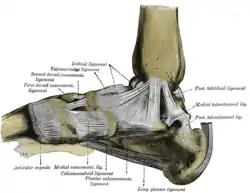 | |
| Calcaneocuboid (bottom center) | |
| Specialty | Orthopedic surgery |
Cuboid syndrome or cuboid subluxation describes a condition that results from subtle injury to the calcaneocuboid joint[1] and ligaments in the vicinity of the cuboid bone, one of seven tarsal bones of the human foot.
This condition often manifests in the form of lateral (little toe side) foot pain and sometimes general foot weakness. Cuboid syndrome, which is relatively common but not well defined or recognized,[2] is known by many other names, including lateral plantar neuritis, cuboid fault syndrome, peroneal cuboid syndrome, dropped cuboid, locked cuboid and subluxed cuboid.[1][3]
Signs and symptoms
A patient with cuboid syndrome usually seeks medical advice and attention complaining of pain, discomfort, or weakness along the lateral aspect of the foot between the fourth and fifth metatarsals and the calcaneocuboid joint.[1] The pain may radiate throughout the foot.[1] Tenderness may be elicited over the tendon of the peroneus longus muscle and an antalgic gait may be observed.[1] The pain may be observed in a controlled environment by standing on the toes or rolling the arches of the foot, as these motions tend to exercise the foot's calcaneocuboid joint and ligament, which are characteristically strained in a patient suffering from cuboid syndrome.[4] Also, the pain may come on suddenly or it may develop gradually and persist over time. Sometimes the pain is intermittent, subsiding partially or completely for a period of time before returning again.[3]
Causes
A patient may develop Cuboid syndrome through either a single traumatic event (e.g., ankle sprain) or insidiously with repetitive strain over time.[1] The exact etiology of Cuboid syndrome remains unclear but many ideas have been proposed. Such ideas include excessive pronation of the foot, overuse injury, and inversion ankle sprains.[1] The favored idea is that the cuboid bone is forcefully everted while the calcaneus is inverted resulting in incongruity at the calcaneocuboid joint.[1] The condition mainly affects athletes, especially those whose activities incur a significant amount of pressure on their feet from jumping or running (such as ballet dancers[5] and runners) and those who place added strain on their feet during lateral maneuvering (such as tennis and basketball players[3][4]). Cuboid syndrome may persist even if the patient is taking part in regular physical therapy.[3] The patient's foot type, such as the presence of overpronation or underpronation, may also play a factor in the condition.
Risk factors
Suspected risk factors for Cuboid syndrome include obesity, midtarsal instability, poorly fitting footwear, physical exercise, inadequate recovery from physical activity, physical training on uneven surfaces, and ankle sprains.[1]
Diagnosis
The underside of the foot comprises the heel, arch and forefoot. There are five bones in the forefoot called metatarsal bones, numbered one to five from the hallux (big toe) to the small toe. These metatarsal bones connect the five phalanges of the foot with the distal aspects of the cuneiform bones and cuboid bone located in the region between the arch and ankle.
By applying soft to medium finger pressure simultaneously on the bottom and top of the forefoot, working along the metatarsal bone 5 from the toe towards the heal, a pain point will be identified at the end of the metatarsal bone at the cuboid joint close to the ankle.
If dull or no pain is experienced, repeat the same procedure along metatarsal bone 4 and subsequently metatarsal bone 3, 2 and 1. Cuboid syndrome usually occurs at the cuboid bone joint connecting metatarsal bone 4 or 5.
Pain may be associated with a sprain, fracture or dislocation and a podiatrist should provide a professional examination, diagnosis and treatment accordingly.
Treatment
Once diagnosed, a medical professional may treat cuboid syndrome by realigning (also known as reducing) the subluxed cuboid unless contraindications to manipulation are present such as gout, inflammatory arthritis, bony disease, neurovascular compromise, or a bone fracture.[1][3] This form of manual manipulation of the foot should be done by a trained specialist, such as an orthopedic surgeon or podiatrist, or secondarily a chiropractor, osteopath, athletic trainer, osteopathic physician, or physical therapist. Further treatment may take into account other considerations, such as possible causes or aggravators (e.g. recommending that the patient be fit with custom orthotics if they are overprone). Fortunately, subluxed cuboids are generally quite treatable[4] and most patients return to a normal level of activity once the pain is brought under control.[3]
See also
References
- 1 2 3 4 5 6 7 8 9 10 Durall, CJ (November 2011). "Examination and treatment of cuboid syndrome: a literature review". Sports Health. 3 (6): 514–519. doi:10.1177/1941738111405965. PMC 3445231. PMID 23016051.
- ↑ Baravarian, Babak (March 2005). "Diagnostic Dilemmas: A Guide To Understanding And Treating Lateral Column Pain". Podiatry Today 18(3). Archived from the original on 2006-03-22. Retrieved 22 June 2020.
- 1 2 3 4 5 6 Caselli, Mark A.; Pantelaras, Nikiforos (October 2004). "How to Treat Cuboid Syndrome in The Athlete". Podiatry Today 17 (10). Archived from the original on 2006-02-21. Retrieved 22 June 2020.
- 1 2 3 Allen, Rick (November 2002). "Subluxated Cuboid Bone" (Reprinted from Instep Dance Magazine). Archived from the original on 2006-05-28. Retrieved June 22, 2020 – via Cascade Wellness Clinic.
- ↑ Marshall, Peter; Hamilton, William G. (1992). "Cuboid subluxation in ballet dancers". The American Journal of Sports Medicine. 20 (2): 169–175. doi:10.1177/036354659202000213.