| Female hysteria | |
|---|---|
 | |
| Women with hysteria under the effects of hypnosis | |
| Specialty | Psychiatry |
Female hysteria was once a common medical diagnosis for women. It was described as exhibiting a wide array of symptoms, including anxiety, shortness of breath, fainting, nervousness, sexual desire, insomnia, fluid retention, heaviness in the abdomen, irritability, loss of appetite for food or sex, even sexually forward behavior, and a "tendency to cause trouble for others".[1] It is no longer recognized by medical authorities as a medical disorder. Its diagnosis and treatment were routine for hundreds of years in Western Europe.[1]
In Western medicine, hysteria was considered both common and chronic among women. Even though it was categorized as a disease, hysteria's symptoms were synonymous with normal functioning female sexuality.[1] In the context of hysteria, every symptom and negative thought was linked to sex.[2] In extreme cases, the woman may have been forced to enter an insane asylum or to undergo surgical hysterectomy.[3]
Early history

The history of hysteria can be traced to ancient times. Dating back to 1900 BC in ancient Egypt, the first descriptions of hysteria within the female body were found recorded on the Kahun Papyri.[4] In this culture, the womb was thought capable of affecting much of the rest of the body, but "there is no warrant for the fanciful view that the ancient Egyptians believed that a variety of bodily complaints were due to an animate, wandering womb".[5] In this time, the medical issue of uterine prolapse was also known.[5]
In ancient Greece, wandering womb was described in the gynecological treatise of the Hippocratic Corpus, "Diseases of Women",[6] which dates back to the 5th and 4th centuries BC. Plato's dialogue Timaeus compares a woman's uterus to a living creature that wanders throughout a woman's body, "blocking passages, obstructing breathing, and causing disease".[7] Aretaeus of Cappadocia described the uterus as "an animal within an animal" (less emotively, "a living thing inside a living thing"), which causes symptoms by wandering around a woman's body putting pressure on other organs.[6] Timaeus also argued that the uterus is "sad and unfortunate" when it does not join with a male or bear child.[4] The standard cure for this "hysterical suffocation" was scent therapy, in which good smells were placed under a woman's genitals and bad odors at the nose, while sneezing could be also induced to drive the uterus back to its correct place.[6] The concept of a pathological "wandering womb" was later viewed as the source of the term hysteria,[7] which stems from the Greek cognate of uterus, ὑστέρα (hystera), although the word hysteria does not feature in ancient Greek medicine: 'the noun is not used in this period'.[7]
While in the Hippocratic texts a wide range of women were susceptible – including in particular the childless – Galen in the 2nd century omitted the childless and saw the most vulnerable group as "widows, and particularly those who previously menstruated regularly, had been pregnant and were eager to have intercourse, but were now deprived of all this" (On the Affected Parts, 6.5).[6] He also denied that the womb could "move from one place to another like a wandering animal".[6] His treatments included scent therapy and sexual intercourse, but also rubbing in ointments to the external genitalia; this was to be performed by midwives, not physicians.[6]
While most Hippocratic writers saw the retention of menstrual blood in the womb as a key problem, for Galen even more serious was the retention of "female seed".[8] This was believed to be thinner than male seed and could be retained in the womb.[7] Hysteria was referred to as "the widow's disease", because the female semen was believed to turn venomous if not released through regular climax or intercourse.[9] If the patient was married, this could be completed by intercourse with their spouse. Other than participating in sexual intercourse, it was thought that fumigating the body with special fragrances would supposedly draw the uterus back to its natural spot in the female body. Foul smells applied to the nose would drive it down, and pleasant scents at the vulva would attract it.[7]
Middle Ages, Renaissance, and the early modern period
Through the Middle Ages, another cause of dramatic symptoms could be found: demonic possession.[10] It was thought that demoniacal forces were attracted to those who were prone to melancholy, particularly to single women and the elderly. When a patient could not be diagnosed or cured of a disease, it was thought that the symptoms of what would now be diagnosed as mental illness, were actually those of someone possessed by the devil.[4] After the 17th century, the correlation of demonic possession and hysteria were gradually discarded and instead was described as behavioral deviance, a medical issue.[11]
In the 16th and 17th centuries, hysteria was still believed to be due to the retention of humour or fluids in the uterus, sexual deprivation, or by the tendency of the uterus to wander around the female body causing irritability and suffocation. Self-treatment such as masturbation, was not recommended and was also considered taboo. Marriage, and regular sexual encounters with her husband, was still the most highly recommended long-term course of treatment for a woman with hysteria.[4][12] It was thought to purge the uterus of any built-up fluid, and semen was thought to have healing properties, In this model, ejaculation outside the vagina was conducive to uterine disease since the female genitalia did not receive the health benefits of male emission. Some physicians regarded all contraceptive practices as injurious to women for this reason. Giovanni Matteo Ferrari da Gradi cited marriage and childbearing as a cure for the disease. If pleasure was obtained from them, then hysteria could be cured.[12] If a woman was unmarried, or widowed, manual stimulation by a midwife involving certain oils and scents was recommended to purge the uterus of any fluid retention. Lack of marriage was also thought to be the cause of most melancholy in single women, such as nuns or widows. Studies of the causes and effects of hysteria were continued in the 16th and 17th century by medical professionals such as Ambroise Pare, Thomas Sydenham, and Abraham Zacuto, who published their findings furthering medical knowledge of the disease, and informing treatment.[12][4] Physician Abraham Zacuto writes in his Praxis Medica Admiranda from 1637,
'Because of retention of the sexual fluid, the heart and surrounding areas are enveloped in a morbid and moist exudation: this is especially true of the more lascivious females, inclined to venery, passionate women who are most eager to experience physical pleasure; if she is of this type she cannot ever be relieved by any aid except that of her parents who are advised to find her a husband. Having done so the man's strong and vigorous intercourse alleviated the frenzy.'
— Maines, 29, [12]
There was continued debate about whether it was morally acceptable for a physician to remove excess female seed through genital manipulation of the female patient; Pieter van Foreest (Forestus) and Giovanni Matteo da Grado (Gradus) insisted on using midwives as intermediaries, and regarded the treatment as the last resort.[13]
18th century
In the 18th century, hysteria slowly became associated with mechanisms in the brain rather than the uterus. This is also when it was noted both men and women could contract hysteria.[14] French physician Philippe Pinel freed hysteria patients detained in Paris' Salpêtrière sanatorium on the basis that kindness and sensitivity were needed to formulate good care. Another French physician, Francois de Sauvages de La Croix believed some common signs of female hysteria were "tears and laughter, oscitation [yawning], pandiculation (stretching and yawning), suffocating angina (chest pain) or dyspnea (shortness of breath), dysphagia (difficulty swallowing), delirium, a close and driving pulse, a swollen abdomen, cold extremities, and abundant and clear urine."[14]
19th century
Jean-Martin Charcot argued that hysteria derived from a neurological disorder and showed that it was more common in men than women.[4] Charcot's theories of hysteria being a physical condition of the mind and not of the body led to a more scientific and analytical approach to hysteria in the 19th century. He dispelled the beliefs that hysteria had anything to do with the supernatural and attempted to define it medically.[15] Charcot's use of photography,[16] and the resulting concretization of women's expressions of health and distress, continued to influence women's experiences of seeking healthcare.[17] Though older ideas persisted during this era, over time female hysteria began to be thought of less as a physical ailment and more of a psychological one.[18]
George Beard, a physician who cataloged an incomplete list including 75 pages of possible symptoms of hysteria,[19] claimed that almost any ailment could fit the diagnosis. Physicians thought that the stress associated with the typical female life at the time caused civilized women to be both more susceptible to nervous disorders and to develop faulty reproductive tracts.[20] One American physician expressed pleasure in the fact that the country was "catching up" to Europe in the prevalence of hysteria.[19]
According to Pierre Roussel and Jean-Jacques Rousseau, femininity was a natural and essential desire for women: "Femininity is for both authors an essential nature, with defined functions, and the disease is explained by the non-fulfillment of natural desire."[4] It was during the industrial revolution and the major development of cities and modern lifestyles that disruption of this natural appetite was thought to cause lethargy or melancholy, leading to hysteria.[4] At the time female patients sought medical practitioners for the massage treatment of hysteria. The rate of hysteria was so great in the socially restrictive industrial period that women were prone to carry smelling salts about their person in case they swooned, reminiscent of Hippocrates' theory of using odors to coerce the uterus back into place. For physicians, manual massage treatment was becoming laborious and time-consuming, and they were seeking a way to increase productivity.[12]
Rachel Maines hypothesized that physicians from the classical era until the early 20th century commonly treated hysteria by manually stimulating the genitals of female patients to the point of orgasm, which was denominated "hysterical paroxysm", and that the inconvenience of this may have motivated the original development of and market for the vibrator.[1] Other hysteria treatments included pregnancy, marriage, heterosexual sex, and the application of smelling oils on female genitals.[21] Although Maines's theory that hysteria was treated by manually stimulating female patients' genitalia to orgasm is widely repeated in the literature on female anatomy and sexuality,[22] some historians dispute Maines's claims regarding the prevalence of this treatment for hysteria and its relevance to the invention of the vibrator, describing them as a distortion of the evidence or that they are only relevant to a very small group.[23][24][25] In 2018, Hallie Lieberman and Eric Schatzberg of Georgia Institute of Technology challenged Maines's claims for the use of electromechanical vibrators to treat hysteria in the 19th century.[26] Maines stated that her theory of the prevalence of masturbation for hysteria and its relevance to the invention of the vibrator is a hypothesis and not proven fact.[22]
Frederick Hollick was a firm believer that a main cause of hysteria was licentiousness present in women.[27]
20th century
In the 1910s, psychiatrist L. E. Emerson was heavily involved in treating patients of hysteria at the Boston Psychopathic Hospital. Emerson published case studies on his patients, who were often "young, single, native-born, and white" and either had been raped or had a lack of healthy sexual relationships.[2] One of his more famous works was a case study of a woman called "Miss A". In the study, Emerson summarized the patient's experience with sexual violence, which he said that most women with hysteria had encountered.[28] Miss A would practice self harm, and Emerson deduced that this practice was a release for the sexual assault she had previously experienced, and substituted for a form of masturbation. Another case study was of Sally Hollis, a woman who often viewed her experience with sexual assault by the terms of her own failing actions and female aggression. Believing the roots of hysteria lay in sexual conflict, Emerson paid attention to the theme of lack of sexual knowledge amongst these women, viewing them as repressed.[2] The lack of sexual knowledge ranged from not knowing what menstruation was, how conception began or what the process of giving birth was.
Some women purposefully sought out the "hysteric" diagnosis because they believed it could provide an answer to what they were experiencing. Most of the patients that Emerson saw were single because they were either young or have purposefully avoided men. Author Elizabeth Lunbeck noted that these women typically fell into three categories. They either withdrew from the heterosexual sphere entirely, despite wanting to participate; they experienced something that was sexually unwanted but would experience guilt over what happened like Sally Hollis; or they were haunted by their sexual traumas in the past.[2] As hysteria was growing into a more prominent diagnosis amongst women, it had led to the police treating any report for sexual assault or rape with skepticism, with the common belief at the time being that "sexual assault is physically impossible without consent.".[2]
Freud and decline of diagnosis
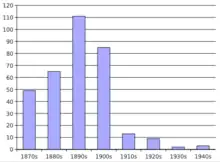
During the early 20th century, the number of women diagnosed with female hysteria sharply declined. Some medical authors claim that the decline was due to gaining a greater understanding of the psychology behind conversion disorders such as hysteria.[29] The understanding of the field of psychiatry was becoming more nuanced at the time, with Sigmund Freud introducing the theory of psychoanalysis, and his other ideas surrounding women and their sexuality.
With so many possible symptoms, historically hysteria was considered a catch-all diagnosis where any unidentifiable ailment could be assigned.[4] As diagnostic techniques improved, the number of ambiguous cases that might have been attributed to hysteria declined. For instance, before the introduction of electroencephalography, epilepsy was frequently confused with hysteria.[30]
Sigmund Freud claimed that hysteria was not anything physical at all but an emotional, internal condition that could affect both males and females, which was caused by previous trauma that led to the affected being unable to enjoy sex in the normal way.[12][15] This would later lead to Freud's development of the Oedipus complex, which connotes femininity as a failure, or lack of masculinity.[15] Although these earlier studies had shown that men were also prone to have hysteria, over time, the condition was related mainly to issues of femininity as the continued study of hysteria took place only in women.[31]
Many cases that had previously been labeled hysteria were reclassified by Freud as anxiety neuroses.[30] It was Freud's theory that hysteria may have been related to the unconscious mind and separate from the conscious mind or the ego.[32] He was convinced that deep conflicts in the mind, some concerning instinctual drives for sex and aggression, were driving the behavior of those with hysteria. The illness of hysteria is a "expression of the impossibility of the fulfillment of the sexual drive because of reminiscence of the Oedipal conflict".[33] This hypothesis is a driving force behind the psychological theory of psychoanalysis, as a way to help patients that had been diagnosed with hysteria reduce internal conflicts causing physical and emotional suffering.
New theories relating to hysteria came from pure speculation; doctors and physicians could not connect symptoms to the disorder, causing it to decline rapidly as a diagnosis.[29] Hysteria was officially taken out of the DSM in 1980.
Today, female hysteria is no longer a recognized illness, but different manifestations of hysteria are recognized in other conditions such as schizophrenia, borderline personality disorder, conversion disorder, and anxiety attacks.[34]
Relationship with women's rights and feminism
In the 1980s, feminists began to reclaim hysteria, using it as a symbol of the systematic oppression of women and reclaiming the term for themselves.[6] The idea of hysteria became an embodiment of the oppressions against women. Especially among sex-positive feminists, who believe sexual repression and having it called hysteria is a form of oppression.[6] The idea stemmed from the belief that Hysteria was a kind of pre-feminist rebellion against the oppressive defined social roles placed upon women. Feminist writers such as Catherine Clément and Hélène Cixous wrote in The Newly Born Woman from a place of opposition to the theories proposed in psychoanalytical works. Clément, Cixous and other feminist writers pushed back against the notion that socially constructed femininities and hysteria are natural to being female.[6][15] Feminist social historians of both sexes argue that hysteria is caused by women's oppressed social roles, rather than by their bodies or psyches, and they have sought its sources in culurrounds healthcare and argues for the fundamental right of care for each and every human.[35]
Representation in creative works
Charlotte Perkins Gilman
"The Yellow Wallpaper" by Charlotte Perkins Gilman is a short story that demonstrates the mistreatment of hysteria and illuminates the deep-rooted misogynistic systems that existed at the time. Published in 1892, this piece is an example of how media around feminist medical care has existed far before modern day. Throughout the story, the female protagonist is confined to an upstairs room at the instruction of her husband who is a physician. Throughout her confinement, the protagonist becomes entranced with the yellow wallpaper. At one point she says there is a woman in it, which is a reflection of her mental state and unreliability as a narrator. The full meaning of the story is up to reader interpretation, but the ending is the outcome of a woman labeled and diagnosed with “hysteria” and not taken seriously by her male husband and male doctors. Through "The Yellow Wallpaper" Perkins shows the lack of care for women's mental health and the condition of hysteria in the late 19th century.
Safe
The 1995 film Safe explores the harmful effects of sexism in healthcare on the psychological and physical health of women and girls. It explores the connections between mental illness, the misdiagnosis of mental illness when physical conditions proved difficult to diagnose, feminism, and healthcare disparities that result from deep-rooted sexism in the medical industry. Both Safe and Gilman's short story, The Yellow Wallpaper explore the differences between the way that men and women experience and view mental illness and healthcare. Similarly, in Fairchild's article “Feminism is now”, she discusses modern misogyny and current examples of sexism in the modern world. The author argues against the idea that feminist goals have already been reached and uncovers how misogyny exists and is visible in many aspects of the lives of women and girls.[36]
See also
References
- 1 2 3 4 Maines, Rachel P. (1999). The Technology of Orgasm: "Hysteria", the Vibrator, and Women's Sexual Satisfaction. Baltimore: The Johns Hopkins University Press. p. 23. ISBN 0-8018-6646-4.
- 1 2 3 4 5 Lunbeck, Elizabeth (11 May 2021), "Hysteria: The Revolt of the "Good Girl"", The Psychiatric Persuasion, Princeton University Press, pp. 209–228, doi:10.2307/j.ctv1h9dgrh.15, retrieved 6 November 2023
- ↑ Mankiller, Wilma P. (1998). The Reader's Companion to U.S. Women's History. Boston, MA: Houghton Mifflin Co. pp. 26. ISBN 0-618-00182-4.
- 1 2 3 4 5 6 7 8 9 Tasca, Cecilia; Rapetti, Mariangela; Carta, Mauro Giovanni; Fadda, Bianca (19 October 2012). "Women And Hysteria In The History Of Mental Health". Clinical Practice and Epidemiology in Mental Health. 8 (1): 110–119. doi:10.2174/1745017901208010110. PMC 3480686. PMID 23115576.
- 1 2 Merskey, Harold; Potter, Paul (1989). "The womb lay still in ancient Egypt". British Journal of Psychiatry. 154 (6): 751–53. doi:10.1192/bjp.154.6.751. PMID 2688786. S2CID 38228923.
- 1 2 3 4 5 6 7 8 9 Gilman, Sander L.; King, Helen; Porter, Roy; Rousseau, G.S.; Showalter, Elaine (1993). Hysteria Beyond Freud. Los Angeles: University of California Press.
- 1 2 3 4 5 King, Helen (1993). "Once upon a text: Hysteria from Hippocrates". In Gilman, Sander; King; Porter, Roy; Rousseau, G.S.; Showalter, Elaine (eds.). Hysteria beyond Freud. University of California Press. p. 25. ISBN 0-520-08064-5.
- ↑ Flemming, Rebecca (2000). Medicine and the Making of Roman Women. Oxford University Press. ISBN 0-19-924002-7.
- ↑ Roach, Mary (2009). Bonk: The Curious Coupling of Science and Sex. New York: W.W. Norton & Co. p. 214. ISBN 978-0-393-33479-1.
- ↑ Brogan, Boyd (2019). "His Belly, Her Seed: Gender and Medicine in Early Modern Demonic Possession". Representations (Berkeley, Calif.). 147 (1): 1–25. doi:10.1525/rep.2019.147.1.1. ISSN 0734-6018. PMC 6814439. PMID 31656366.
- ↑ Spanos, Gottlieb, Nicholas, Jack (1979). "Demonic possession, mesmerism, and hysteria: A social psychological perspective on their historical interrelations". Journal of Abnormal Psychology. 88 (5): 527–546. doi:10.1037/0021-843X.88.5.527. PMID 387849.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - 1 2 3 4 5 6 Maines, Rachel (1999). The technology of Orgasm: 'Hysteria', the Vibrator, and Women's Sexual Satisfaction. Baltimore: The Johns Hopkins University Press.
- ↑ Schleiner, Winfried (1995). Medical Ethics in the Renaissance. Georgetown University Press. p. 115.
- 1 2 Cohut, Maria (13 October 2020). "Female hysteria: The history of a controversial 'condition'". Medical News Today.
- 1 2 3 4 Devereux, Cecily (2014). "Hysteria, Feminism, and Gender Revisited: The Case of the Second Wave". English Studies in Canada. 40 (1): 19–45. doi:10.1353/esc.2014.0004. S2CID 162808510.
- ↑ Goetz, C.G. (1991). "Visual art in the neurologic career of Jean-Martin Charcot". Archives of Neurology. 48 (4): 421–25. doi:10.1001/archneur.1991.00530160091020. PMID 2012518.
- ↑ Jones, A. (2010). The Feminism and Visual Culture Reader. New York: Routledge. pp. 248–58, 300–08.
- ↑ Simon, Matt (7 May 2014). "Fantastically Wrong: The Theory of the Wandering Wombs That Drove Women to Madness". Wired. Retrieved 28 November 2014.
- 1 2 Briggs L (2000). "The race of hysteria: "overcivilization" and the "savage" woman in late nineteenth-century obstetrics and gynecology". American Quarterly. 52 (2): 246–73. doi:10.1353/aq.2000.0013. PMID 16858900. S2CID 8047730.
- ↑ Morantz RM, Zschoche S (December 1980). "Professionalism, feminism, and gender roles: a comparative study of nineteenth-century medical therapeutics". Journal of American History. 67 (3): 568–88. doi:10.2307/1889868. JSTOR 1889868. PMID 11614687.
- ↑ "Medical Vibrators for Treatment of Female Hysteria | The Embryo Project Encyclopedia". embryo.asu.edu. Retrieved 2 April 2021.
- 1 2 Maines, Rachel. "Big Think Interview with Rachel Maines". bigthink.com. Retrieved 16 November 2016.
- ↑ King, Helen (16 December 2011). "Galen and the widow: towards a history of therapeutic masturbation in ancient gynaecology" (PDF). EuGeStA. 1: 205–235.
- ↑ Hall, Lesley. "Doctors masturbating women as a cure for hysteria/'Victorian vibrators'". lesleyahall.net. Retrieved 29 October 2016.
- ↑ Riddell, Fern (10 November 2014). "No, no, no! Victorians didn't invent the vibrator". The Guardian. Retrieved 29 October 2016.
- ↑ Lieberman, Hallie; Schatzberg, Eric (August 2018). "A failure of academic quality control: The technology of orgasm". Journal of Positive Sexuality. 4 (2): 24–47. doi:10.51681/1.421.
- ↑ Hollick, Frederick (1856). The Diseases of Woman, Their Causes and Cure Familiarly Explained: With Practical Hints for Their Prevention, and for the Preservation of Female Health. T. W. Strong. OCLC 1102679349.
- ↑ Emerson, L. E. (1913). "A psychoanalytic study of a severe case of hysteria". The Journal of Abnormal Psychology.
- 1 2 3 Micale MS (1993). "On the "disappearance" of hysteria. A study in the clinical deconstruction of a diagnosis". Isis; an International Review Devoted to the History of Science and Its Cultural Influences. 84 (3): 496–526. doi:10.1086/356549. JSTOR 235644. PMID 8282518. S2CID 37252994.
- 1 2 Micale, M. S. (July 2000). "The decline of hysteria". The Harvard Mental Health Letter. 17 (1): 4–6. OCLC 119217716. PMID 10877868.
- ↑ "The History of Hysteria: Sexism in Diagnosis". 2017.
- ↑ Coon, Mitterer, Dennis, John (2013). Introduction to Psychology: Gateways to Mind and Behavior. Cengage Learning. pp. 512–513.
{{cite book}}: CS1 maint: multiple names: authors list (link) - ↑ Tasca, Cecilia; Rapetti, Mariangela; Carta, Mauro Giovanni; Fadda, Bianca (2012). "Women and hysteria in the history of mental health". Clinical Practice and Epidemiology in Mental Health. 8: 110–119. doi:10.2174/1745017901208010110. ISSN 1745-0179. PMC 3480686. PMID 23115576.
- ↑ Costa, Dayse Santos; Lang, Charles Elias (2016). "Hysteria Today, Why?". Psicologia USP. 27 (1): 115–124. doi:10.1590/0103-656420140039.
- ↑ Small, Raia (2016). "I Woke Up Like This: Johanna Hedva's Sick Woman Theory". Make/Shift. No. 19. pp. 22–23, 26. ProQuest 1917629527.
- ↑ Fairchild, Kimberly (1 November 2015). "Feminism is Now: Fighting Modern Misogyny and the Myth of the Post-Feminist Era". Sex Roles. 73 (9): 453–455. doi:10.1007/s11199-015-0524-7. ISSN 1573-2762. S2CID 255012952.
Further reading
- Fairchild, Kimberly (November 2015). "Feminism is Now: Fighting Modern Misogyny and the Myth of the Post-Feminist Era: Modern Misogyny: Anti-Feminism in a Post-Feminist Era. By Kristin J. Anderson, New York, Oxford University Press, 2014. 183 pp. $29.95 (paperback). ISBN: 978-0-19-932817-8". Sex Roles. 73 (9–10): 453–455. doi:10.1007/s11199-015-0524-7. S2CID 255012952.
- Spurgas, Alyson K. (2020). Diagnosing Desire: Biopolitics and Femininity Into the Twenty-first Century. Ohio State University Press. ISBN 978-0-8142-1451-0.
- Katz, James D.; Seaman, Rachel; Diamond, Shari (May 2008). "Exposing Gender Bias in Medical Taxonomy: Toward Embracing a Gender Difference Without Disenfranchising Women". Women's Health Issues. 18 (3): 151–154. doi:10.1016/j.whi.2008.03.002. PMID 18457752.
- Hedva, Johanna (2020). "Sick Woman Theory" (PDF).
- Suslovic, Brianna (2 January 2023). "Hysterical Solidarity: An Embodied Reflection on Contemporary Sexual and Reproductive Rights Concerns in the United States". Studies in Gender and Sexuality. 24 (1): 21–27. doi:10.1080/15240657.2022.2161284. S2CID 257535669.
- Greenhalgh, Ally (6 December 2022). "Medicine and Misogyny: The Misdiagnosis of Women". Confluence.
- Villines, Zawn (25 October 2021). "Gender bias in healthcare: Examples and consequences". Medical News Today.
- Jackson, Zakiyyah Iman (2020). Becoming Human. doi:10.18574/nyu/9781479890040.001.0001. ISBN 978-1-4798-3455-6. S2CID 261359346.
- Mickles, Kiana (October 2017). "Beyond J. Marion Sims: Black Women Have Been Fighting Discrimination in the Medical Industrial Complex for Centuries". CRWNMAG.
- Kapsalis, Terri (2008). The Hysterical Alphabet. WhiteWalls. ISBN 978-0-945323-16-7.
- Libbrecht, Katrien (1995). Hysterical Psychosis: A Historical Survey. London: Transaction Publishers. ISBN 1-56000-181-X.
- Micale, Mark S. (1995). Approaching Hysteria: Disease and its Interpretations. Princeton University Press. ISBN 0-691-03717-5.
- Micale, Mark S. (2009). Hysterical Men: The Hidden History of Male Nervous Illness. Harvard University Press. ISBN 978-0-674-04098-4.
- Micklem, Niel (1996). The Nature of Hysteria. Routledge. ISBN 0-415-12186-8.
- Bronfen, Elisabeth (2014). The Knotted Subject: Hysteria and Its Discontents. Princeton University Press. ISBN 978-1-4008-6473-7.
- Augsburg, Tanya (1996). Private Theatres Onstage (Hysteria and the Female Medical Subject). UMI.
- Showalter, Elaine (1987). The Female Malady: Women, Madness and English Culture, 1830-1980. Virago. ISBN 978-0-86068-869-3.
- Lewis Herman, Judith (1992). Trauma and Recovery: The Aftermath of Violence--From Domestic Abuse to Political Terror. Basic Books. ISBN 978-0-465-08730-3.
External links
- Erika Kinetz, "Is Hysteria Real? Brain Images Say Yes" (The New York Times)
- Female Hysteria during Victorian Era