| Typical antipsychotic | |
|---|---|
| Drug class | |
 Skeletal formula of chlorpromazine, the first neuroleptic drug | |
| Synonyms | First generation antipsychotics, conventional antipsychotics, classical neuroleptics, traditional antipsychotics, major tranquilizers |
| Legal status | |
| In Wikidata | |
Typical antipsychotics (also known as major tranquilizers, and first generation antipsychotics) are a class of antipsychotic drugs first developed in the 1950s and used to treat psychosis (in particular, schizophrenia). Typical antipsychotics may also be used for the treatment of acute mania, agitation, and other conditions. The first typical antipsychotics to come into medical use were the phenothiazines, namely chlorpromazine which was discovered serendipitously.[1] Another prominent grouping of antipsychotics are the butyrophenones, an example of which is haloperidol. The newer, second-generation antipsychotics, also known as atypical antipsychotics, have largely supplanted the use of typical antipsychotics as first-line agents due to the higher risk of movement disorders in the latter.
Both generations of medication tend to block receptors in the brain's dopamine pathways, but atypicals at the time of marketing were claimed to differ from typical antipsychotics in that they are less likely to cause extrapyramidal symptoms (EPS), which include unsteady Parkinson's disease-type movements, internal restlessness, and other involuntary movements (e.g. tardive dyskinesia, which can persist after stopping the medication).[2] More recent research has demonstrated the side effect profile of these drugs is similar to older drugs, causing the leading medical journal The Lancet to write in its editorial "the time has come to abandon the terms first-generation and second-generation antipsychotics, as they do not merit this distinction."[3] While typical antipsychotics are more likely to cause EPS, atypicals are more likely to cause adverse metabolic effects, such as weight gain and increase the risk for type II diabetes.[4]
Clinical uses
Typical antipsychotics block the dopamine 2 receptor (D2) receptor, causing a tranquilizing effect.[5] It is thought that 60–80% of D2 receptors need to be occupied for antipsychotic effect.[5] For reference, the typical antipsychotic haloperidol tends to block about 80% of D2 receptors at doses ranging from 2 to 5 mg per day.[5] On the aggregate level, no typical antipsychotic is more effective than any other, though people will vary in which antipsychotic they prefer to take based on individual differences in tolerability and effectiveness.[5] Typical antipsychotics can be used to treat, e.g., schizophrenia or severe agitation.[5] Haloperidol, due to the availability of a rapid-acting injectable formulation and decades of use, remains the most commonly used antipsychotic for treating severe agitation in the emergency department setting.[5]
Adverse effects
Adverse effects vary among the various agents in this class of medications, but common effects include: dry mouth, muscle stiffness, muscle cramping, tremors, EPS and weight gain. EPS refers to a cluster of symptoms consisting of akathisia, parkinsonism, and dystonia. Anticholinergics such as benztropine and diphenhydramine are commonly prescribed to treat the EPS. 4% of users develop rabbit syndrome while on typical antipsychotics.[6]
There is a risk of developing a serious condition called tardive dyskinesia as a side effect of antipsychotics, including typical antipsychotics. The risk of developing tardive dyskinesia after chronic typical antipsychotic usage varies on several factors, such as age and gender, as well as the specific antipsychotic used. The commonly reported incidence of TD among younger patients is about 5% per year. Among older patients incidence rates as high as 20% per year have been reported. The average prevalence is approximately 30%.[7] There are few treatments that have consistently been shown to be effective for the treatment of tardive dyskinesia, though an VMAT2 inhibitor like valbenazine may help.[8] The atypical antipsychotic clozapine has also been suggested as an alternative antipsychotic for patients experiencing tardive dyskinesia.[9] Tardive dyskinesia may reverse upon discontinuation of the offending agent or it may be irreversible, withdrawal may also make tardive dyskinesia more severe.[10]
Neuroleptic malignant syndrome (NMS) is a rare, but potentially fatal side effect of antipsychotic treatment. NMS is characterized by fever, muscle rigidity, autonomic dysfunction, and altered mental status. Treatment includes discontinuation of the offending agent and supportive care.
The role of typical antipsychotics has come into question recently as studies have suggested that typical antipsychotics may increase the risk of death in elderly patients. A 2005 retrospective cohort study from the New England Journal of Medicine showed an increase in risk of death with the use of typical antipsychotics that was on par with the increase shown with atypical antipsychotics.[11] This has led some to question the common use of antipsychotics for the treatment of agitation in the elderly, particularly with the availability of alternatives such as mood stabilizing and antiepileptic drugs.
Potency
Traditional antipsychotics are classified as high-potency, mid-potency, or low-potency based on their potency for the D2 receptor:
| Potency | Examples | Adverse effect profile |
| high | fluphenazine and haloperidol | more extrapyramidal side effects (EPS) and less antihistaminic effects (e.g. sedation), alpha adrenergic antagonism (e.g. orthostatic hypotension), and anticholinergic effects (e.g. dry mouth) |
| middle | perphenazine and loxapine | intermediate D2 affinity, with more off-target effects than high-potency agents |
| low | chlorpromazine | less risk of EPS but more antihistaminic effects, alpha adrenergic antagonism, and anticholinergic effects |
Prochlorperazine (Compazine, Buccastem, Stemetil) and Pimozide (Orap) are less commonly used to treat psychotic states, and so are sometimes excluded from this classification.[12]
A related concept to D2 potency is the concept of "chlorpromazine equivalence", which provides a measure of the relative effectiveness of antipsychotics.[13][14] The measure specifies the amount (mass) in milligrams of a given drug that must be administered in order to achieve desired effects equivalent to those of 100 milligrams of chlorpromazine.[15] Another method is "defined daily dose" (DDD), which is the assumed average dose of an antipsychotic that an adult would receive during long-term treatment.[15] DDD is primarily used for comparing the utilization of antipsychotics (e.g. in an insurance claim database), rather than comparing therapeutic effects between antipsychotics.[15] Maximum dose methods are sometimes used to compare between antipsychotics as well.[15] It is important to note that these methods do not generally account for differences between the tolerability (i.e. the risk of side effects) or the safety between medications.[15]
For a list of typical antipsychotics organized by potency, see below:
Low potency
- Chlorpromazine
- Chlorprothixene
- Levomepromazine
- Mesoridazine
- Periciazine
- Promazine
- Thioridazine† (withdrawn by brand-name manufacturer and most countries)
Medium potency
High potency
- Droperidol
- Flupentixol
- Fluphenazine
- Haloperidol
- Pimozide
- Prochlorperazine
- Thioproperazine
- Trifluoperazine
- Zuclopenthixol
Where: † indicates products that have since been discontinued.[16]
Long-acting injectables
Some typical antipsychotics have been formulated as a long-acting injectable (LAI), or "depot", formulation. Depot injections are also used on persons under involuntary commitment to force compliance with a court treatment order when the person would refuse to take daily oral medication. This has the effect of dosing a person who doesn't consent to take the drug. The United Nations Special Rapporteur On Torture has classified this as a human rights violation and cruel or inhuman treatment.[17]
The first LAI antipsychotics (often referred to as simply "LAIs") were the typical antipsychotics fluphenazine and haloperidol.[18] Both fluphenazile and haloperidol are formulated as decanoates, referring to the attachment of a decanoic acid group to the antipsychotic molecule.[18] These are then dissolved in an organic oil.[18] Together, these modifications prevent the active medications from being released immediately upon injection, attaining a slow release of the active medications (note, though, that the fluphenazine decanoate product is unique for reaching peak fluphenazine blood levels within 24 hours after administration[19]).[18] Fluphenazine decanoate can be administered every 7 to 21 days (usually every 14 to 28 days),[19] while haloperidol decanoate can be administered every 28 days, though some people receive more or less frequent injections.[18] If a scheduled injection of either haloperidol decanoate or fluphenazine decanoate is missed, recommendations for administering make-up injectable dose(s) or providing antipsychotics to be taken by mouth vary by, e.g., how long ago the last injection was and how many previous injections the person has received (i.e., if steady state levels of the medication have been reached or not).[19]
Both of the typical antipsychotic LAIs are inexpensive in comparison to the atypical LAIs.[18] Doctors usually prefer atypical LAIs over typical LAIs due to the differences in adverse effects between typical and atypical antipsychotics in general.[19]
| Medication | Brand name | Class | Vehicle | Dosage | Tmax | t1/2 single | t1/2 multiple | logPc | Ref |
|---|---|---|---|---|---|---|---|---|---|
| Aripiprazole lauroxil | Aristada | Atypical | Watera | 441–1064 mg/4–8 weeks | 24–35 days | ? | 54–57 days | 7.9–10.0 | |
| Aripiprazole monohydrate | Abilify Maintena | Atypical | Watera | 300–400 mg/4 weeks | 7 days | ? | 30–47 days | 4.9–5.2 | |
| Bromperidol decanoate | Impromen Decanoas | Typical | Sesame oil | 40–300 mg/4 weeks | 3–9 days | ? | 21–25 days | 7.9 | [20] |
| Clopentixol decanoate | Sordinol Depot | Typical | Viscoleob | 50–600 mg/1–4 weeks | 4–7 days | ? | 19 days | 9.0 | [21] |
| Flupentixol decanoate | Depixol | Typical | Viscoleob | 10–200 mg/2–4 weeks | 4–10 days | 8 days | 17 days | 7.2–9.2 | [21][22] |
| Fluphenazine decanoate | Prolixin Decanoate | Typical | Sesame oil | 12.5–100 mg/2–5 weeks | 1–2 days | 1–10 days | 14–100 days | 7.2–9.0 | [23][24][25] |
| Fluphenazine enanthate | Prolixin Enanthate | Typical | Sesame oil | 12.5–100 mg/1–4 weeks | 2–3 days | 4 days | ? | 6.4–7.4 | [24] |
| Fluspirilene | Imap, Redeptin | Typical | Watera | 2–12 mg/1 week | 1–8 days | 7 days | ? | 5.2–5.8 | [26] |
| Haloperidol decanoate | Haldol Decanoate | Typical | Sesame oil | 20–400 mg/2–4 weeks | 3–9 days | 18–21 days | 7.2–7.9 | [27][28] | |
| Olanzapine pamoate | Zyprexa Relprevv | Atypical | Watera | 150–405 mg/2–4 weeks | 7 days | ? | 30 days | – | |
| Oxyprothepin decanoate | Meclopin | Typical | ? | ? | ? | ? | ? | 8.5–8.7 | |
| Paliperidone palmitate | Invega Sustenna | Atypical | Watera | 39–819 mg/4–12 weeks | 13–33 days | 25–139 days | ? | 8.1–10.1 | |
| Perphenazine decanoate | Trilafon Dekanoat | Typical | Sesame oil | 50–200 mg/2–4 weeks | ? | ? | 27 days | 8.9 | |
| Perphenazine enanthate | Trilafon Enanthate | Typical | Sesame oil | 25–200 mg/2 weeks | 2–3 days | ? | 4–7 days | 6.4–7.2 | [29] |
| Pipotiazine palmitate | Piportil Longum | Typical | Viscoleob | 25–400 mg/4 weeks | 9–10 days | ? | 14–21 days | 8.5–11.6 | [22] |
| Pipotiazine undecylenate | Piportil Medium | Typical | Sesame oil | 100–200 mg/2 weeks | ? | ? | ? | 8.4 | |
| Risperidone | Risperdal Consta | Atypical | Microspheres | 12.5–75 mg/2 weeks | 21 days | ? | 3–6 days | – | |
| Zuclopentixol acetate | Clopixol Acuphase | Typical | Viscoleob | 50–200 mg/1–3 days | 1–2 days | 1–2 days | 4.7–4.9 | ||
| Zuclopentixol decanoate | Clopixol Depot | Typical | Viscoleob | 50–800 mg/2–4 weeks | 4–9 days | ? | 11–21 days | 7.5–9.0 | |
| Note: All by intramuscular injection. Footnotes: a = Microcrystalline or nanocrystalline aqueous suspension. b = Low-viscosity vegetable oil (specifically fractionated coconut oil with medium-chain triglycerides). c = Predicted, from PubChem and DrugBank. Sources: Main: See template. | |||||||||
History
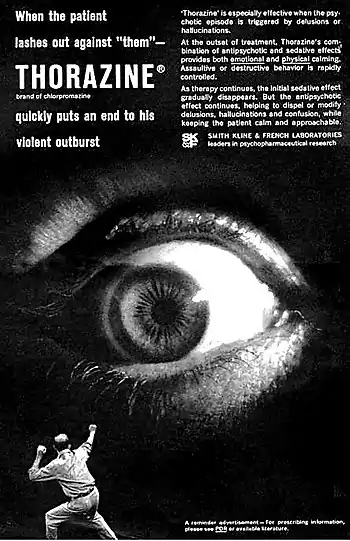
The original antipsychotic drugs were happened upon largely by chance and then tested for their effectiveness. The first, chlorpromazine, was developed as a surgical anesthetic after an initial report in 1952.[5] It was first used in psychiatric institutions because of its powerful tranquilizing effect; at the time it was advertised as a "pharmacological lobotomy".[31] (Note that "tranquilizing" here only refers to changes in external behavior, while the experience a person has internally may be one of increased agitation but inability to express it.)[32]
Until the 1970s there was considerable debate within psychiatry on the most appropriate term to use to describe the new drugs.[33] In the late 1950s the most widely used term was "neuroleptic", followed by "major tranquilizer" and then "ataraxic".[33] The word neuroleptic was coined in 1955 by Delay and Deniker after their discovery (1952) of the antipsychotic effects of chlorpromazine.[33] It is derived from the Greek: "νεῦρον" (neuron, originally meaning "sinew" but today referring to the nerves) and "λαμβάνω" (lambanō, meaning "take hold of"). Thus, the word means taking hold of one's nerves. It was often taken to refer also to common effects such as reduced activity in general, as well as lethargy and impaired motor control. Although these effects are unpleasant and harmful, they were, along with akathisia, considered a reliable sign that the drug was working.[31] These terms have been largely replaced by the term "antipsychotic" in medical and advertising literature, which refers to the medication's more-marketable effects.[33]
See also
References
- ↑ Shen WW (1999). "A history of antipsychotic drug development". Comprehensive Psychiatry. 40 (6): 407–14. doi:10.1016/s0010-440x(99)90082-2. PMID 10579370.
- ↑ "A roadmap to key pharmacologic principles in using antipsychotics". Primary Care Companion to the Journal of Clinical Psychiatry. 9 (6): 444–54. 2007. doi:10.4088/PCC.v09n0607. PMC 2139919. PMID 18185824.
- ↑ Tyrer P, Kendall T (January 2009). "The spurious advance of antipsychotic drug therapy". Lancet. 373 (9657): 4–5. doi:10.1016/S0140-6736(08)61765-1. PMID 19058841. S2CID 19951248. Archived from the original on 2023-02-06. Retrieved 2023-03-02.
- ↑ "Not found". www.rcpsych.ac.uk. Archived from the original on 8 May 2018. Retrieved 8 May 2018.
- 1 2 3 4 5 6 7 Schatzberg's Manual of Clinical Psychopharmacology (Ninth ed.). American Psychiatric Association Publishing. 2019. ISBN 978-1-61537-230-0.
- ↑ Yassa R, Lal S (May 1986). "Prevalence of the rabbit syndrome". The American Journal of Psychiatry. 143 (5): 656–7. doi:10.1176/ajp.143.5.656. PMID 2870650.
- ↑ Llorca PM, Chereau I, Bayle FJ, Lancon C (May 2002). "Tardive dyskinesias and antipsychotics: a review". European Psychiatry. 17 (3): 129–38. doi:10.1016/S0924-9338(02)00647-8. PMID 12052573. S2CID 40761404.
- ↑ Office of the Commissioner (24 March 2020). "FDA approves first drug to treat tardive dyskinesia". FDA. Retrieved 18 June 2020.
- ↑ Pardis P, Remington G, Panda R, Lemez M, Agid O (October 2019). "Clozapine and tardive dyskinesia in patients with schizophrenia: A systematic review". Journal of Psychopharmacology. 33 (10): 1187–1198. doi:10.1177/0269881119862535. PMID 31347436. S2CID 198912192.
- ↑ "Tardive dyskinesia: MedlinePlus Medical Encyclopedia". Archived from the original on 2017-01-31. Retrieved 2017-01-18.
- ↑ Wang PS, Schneeweiss S, Avorn J, Fischer MA, Mogun H, Solomon DH, Brookhart MA (December 2005). "Risk of death in elderly users of conventional vs. atypical antipsychotic medications". The New England Journal of Medicine. 353 (22): 2335–41. doi:10.1056/NEJMoa052827. PMID 16319382. S2CID 35202051.
- ↑ Gitlin MJ (1996). The psychotherapist's guide to psychopharmacology. New York: Free Press. p. 392. ISBN 0-684-82737-9.
- ↑ Woods SW (June 2003). "Chlorpromazine equivalent doses for the newer atypical antipsychotics". The Journal of Clinical Psychiatry. 64 (6): 663–7. doi:10.4088/JCP.v64n0607. PMID 12823080.
- ↑ Rijcken CA, Monster TB, Brouwers JR, de Jong-van den Berg LT (December 2003). "Chlorpromazine equivalents versus defined daily doses: how to compare antipsychotic drug doses?". Journal of Clinical Psychopharmacology. 23 (6): 657–9. doi:10.1097/01.jcp.0000096247.29231.3a. PMID 14624195. S2CID 12939895.
- 1 2 3 4 5 Patel MX, Arista IA, Taylor M, Barnes TR (September 2013). "How to compare doses of different antipsychotics: a systematic review of methods". Schizophrenia Research. 149 (1–3): 141–8. doi:10.1016/j.schres.2013.06.030. PMID 23845387. S2CID 45642900.
- ↑ Martindale: The Complete Drug Reference. The Royal Pharmaceutical Society of Great Britain. 2013. Retrieved 2 November 2013.
- ↑ https://www.madinamerica.com/wp-content/uploads/2013/03/torture.pdf
- 1 2 3 4 5 6 Kennedy WK (2012). "When and how to use long-acting injectable antipsychotics". Current Psychiatry. 11 (8): 40–43.
- 1 2 3 4 Carpenter J, Wong KK (2018). "Long-acting injectable antipsychotics: What to do about missed doses". Current Psychiatry. 17 (7): 10–12, 14–19, 56.
- ↑ Parent M, Toussaint C, Gilson H (1983). "Long-term treatment of chronic psychotics with bromperidol decanoate: clinical and pharmacokinetic evaluation". Current Therapeutic Research. 34 (1): 1–6.
- 1 2 Jørgensen A, Overø KF (1980). "Clopenthixol and flupenthixol depot preparations in outpatient schizophrenics. III. Serum levels". Acta Psychiatrica Scandinavica. Supplementum. 279: 41–54. doi:10.1111/j.1600-0447.1980.tb07082.x. PMID 6931472.
- 1 2 Reynolds JE (1993). "Anxiolytic sedatives, hypnotics and neuroleptics.". Martindale: The Extra Pharmacopoeia (30th ed.). London: Pharmaceutical Press. pp. 364–623.
- ↑ Ereshefsky L, Saklad SR, Jann MW, Davis CM, Richards A, Seidel DR (May 1984). "Future of depot neuroleptic therapy: pharmacokinetic and pharmacodynamic approaches". The Journal of Clinical Psychiatry. 45 (5 Pt 2): 50–9. PMID 6143748.
- 1 2 Curry SH, Whelpton R, de Schepper PJ, Vranckx S, Schiff AA (April 1979). "Kinetics of fluphenazine after fluphenazine dihydrochloride, enanthate and decanoate administration to man". British Journal of Clinical Pharmacology. 7 (4): 325–31. doi:10.1111/j.1365-2125.1979.tb00941.x. PMC 1429660. PMID 444352.
- ↑ Young D, Ereshefsky L, Saklad SR, Jann MW, Garcia N (1984). Explaining the pharmacokinetics of fluphenazine through computer simulations. (Abstract.). 19th Annual Midyear Clinical Meeting of the American Society of Hospital Pharmacists. Dallas, Texas.
- ↑ Janssen PA, Niemegeers CJ, Schellekens KH, Lenaerts FM, Verbruggen FJ, van Nueten JM, et al. (November 1970). "The pharmacology of fluspirilene (R 6218), a potent, long-acting and injectable neuroleptic drug". Arzneimittel-Forschung. 20 (11): 1689–98. PMID 4992598.
- ↑ Beresford R, Ward A (January 1987). "Haloperidol decanoate. A preliminary review of its pharmacodynamic and pharmacokinetic properties and therapeutic use in psychosis". Drugs. 33 (1): 31–49. doi:10.2165/00003495-198733010-00002. PMID 3545764.
- ↑ Reyntigens AJ, Heykants JJ, Woestenborghs RJ, Gelders YG, Aerts TJ (1982). "Pharmacokinetics of haloperidol decanoate. A 2-year follow-up". International Pharmacopsychiatry. 17 (4): 238–46. doi:10.1159/000468580. PMID 7185768.
- ↑ Larsson M, Axelsson R, Forsman A (1984). "On the pharmacokinetics of perphenazine: a clinical study of perphenazine enanthate and decanoate". Current Therapeutic Research. 36 (6): 1071–88.
- ↑ The text reads: "When the patient lashes out against 'them' - THORAZINE (brand of chlorpromazine) quickly puts an end to his violent outburst. 'Thorazine' is especially effective when the psychotic episode is triggered by delusions or hallucinations. At the outset of treatment, Thorazine's combination of antipsychotic and sedative effects provides both emotional and physical calming. Assaultive or destructive behavior is rapidly controlled. As therapy continues, the initial sedative effect gradually disappears. But the antipsychotic effect continues, helping to dispel or modify delusions, hallucinations and confusion, while keeping the patient calm and approachable. SMITH KLINE AND FRENCH LABORATORIES leaders in psychopharmaceutical research."
- 1 2 Pieters T, Majerus B (December 2011). "The introduction of chlorpromazine in Belgium and the Netherlands (1951-1968); tango between old and new treatment features". Studies in History and Philosophy of Biological and Biomedical Sciences. 42 (4): 443–52. doi:10.1016/j.shpsc.2011.05.003. PMID 22035718. Archived from the original on 9 July 2017.
- ↑ Muench, John (1 March 2010). "Adverse Effects Of Antipsychotics". American Family Physician. 81 (5): 617–622. Retrieved 23 March 2021.
- 1 2 3 4 King C, Voruganti LN (May 2002). "What's in a name? The evolution of the nomenclature of antipsychotic drugs". Journal of Psychiatry & Neuroscience. 27 (3): 168–75. PMC 161646. PMID 12066446.