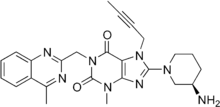
利格列汀
利格列汀(INN:),或称利拉利汀,屬於新一代DPP-4抑制劑(dipeptidyl peptidase (DPP)-4 inhibitors)的糖尿病藥物,於2011年5月獲美國食品及藥物管理局(FDA)核准,在配合飲食及運動下,用於治療成年人二型糖尿病[1]。「利格列汀」是目前唯一一種非主經腎臟排出體外的DPP-4抑制劑口服抗糖尿病藥。多項研究發現,只有5% 的「利格列汀」藥物由腎臟排出[2],其餘大部分未經代謝的藥物會由膽汁及腸道排泄出來,並不如其他同類口服糖尿病藥物(如﹕Sitagliptin「西他列汀」、Vildagliptin「維格列汀」及Saxagliptin「沙格列汀」) 有近7成至9成經腎臟排出 [3][4][5][6] 。
 | |
| 臨床資料 | |
|---|---|
| 商品名 | Tradjenta, Trajenta |
| AHFS/Drugs.com | 消费者药物信息 |
| MedlinePlus | a611036 |
| 核准狀況 |
|
| 给药途径 | Oral |
| ATC碼 | |
| 法律規範狀態 | |
| 法律規範 |
|
| 藥物動力學數據 | |
| 生物利用度 | 30% oral |
| 血漿蛋白結合率 | 75% to 99% in plasma |
| 识别 | |
| |
| CAS号 | 668270-12-0 |
| PubChem CID | |
| IUPHAR/BPS | |
| ChemSpider | |
| UNII | |
| KEGG | |
| ChEMBL | |
| 化学 | |
| 化学式 | C25H28N8O2 |
| 摩尔质量 | 472.54 g/mol |
| 3D模型(JSmol) | |
| |
| |
「利格列汀」由德國藥廠研發,與美國藥廠共同推廣,商品名為Trajenta,中文商品則名為 「糖漸平」(台灣) 、「糖安達」(香港)或「歐唐寧」(中國大陸)。
作用機制
二肽基肽酶-4(DPP-4)是人體酵素的一種,能迅速分解兩種腸促胰島素,包括胰升糖素樣肽(GLP-1)及腸抑胃肽(GIP)。GLP-1和GIP的功能,是刺激胰臟beta細胞製造及分泌胰島素,特別是在進食後血糖水平升高時。GLP-1還有另一項功能,就是抑制胰臟alpha細胞分泌胰升糖素,從而減少肝糖的製造。因此,作為DPP-4抑制劑,「利格列汀」(linagliptin) 能夠在血糖濃度高時黏附於DPP-4上,阻止其分解腸促胰島素[7],延長GLP-1和GIP的壽命,從而促進胰島素分泌,降低胰升糖素水平,改善血糖控制。
DPP-4抑制劑標誌着二型糖尿病治療的一個創新方向,作用機制獨特,與其他類型的二型糖尿病藥物有別。
臨床研究

「利格列汀」(linagliptin)已完成第三期臨床試驗計劃,以証實單獨治療及合併其他常用抗糖尿病藥(例如甲福明、磺胺脲類或格列酮類)的療效、安全性與耐受性。整個計劃的試驗中心分佈全球約40個國家,共納入超過5,000名二型糖尿病病人,當中有過千名病人患有不同程度的腎功能受損,因此臨床試驗計劃中亦包括兩項獨立的長期研究,集中評估「利格列汀」對治療輕度、中度及重度腎功能受損的二型糖尿病病人的安全性及療效[8] [9][10][11][12] [13][14][15][16]。
療效
整體研究結果顯示[8] [9][10][11][12] [13][14][15],無論單獨治療或合併其他抗糖尿病藥物如甲福明、磺胺脲類或格列酮類,「利格列汀」(linagliptin)的控糖療效均十分顯著、持久而且具臨床意義。八項隨機對照研究共納入5,239名二型糖尿病病人,評估「利格列汀」的療效和安全性。共有3,319名二型糖尿病病人接受「利格列汀」治療,當中929名年齡65歲或以上;1,238名患有輕度腎功能受損;143名患有中度腎功能受損。結果證實,每天一次「利格列汀」能顯著改善血糖控制,對病人體重並沒有造成具臨床意義的影響。所有子群組(性別、年齡、腎功能受損程度、體重指數)的糖化血紅素下降幅度相若。
部分研究更發現 ,「利格列汀」能大幅改善beta細胞的功能(beta細胞負責製造及分泌胰島素)[10][11][12] [13][17]。
另外一項為期逾兩年的長期研究[16],比較「利格列汀」或格列美脲加入甲福明治療後的效果12。結果顯示,「利格列汀」能有效降糖,療效不但與格列美脲相若,而且不會引致體重上升,出現血糖過低的風險較格列美脲低,發生心血 管事件的情況也較少。目前的臨床研究証實「利格列汀」有以下的特點:
- 持久穩定血糖至理想目標,具有臨床意義
- 安全性及耐受性良好,血糖過低的風險相當低
- 不會引致體重上升
- 無須調節藥物劑量。即使服用者同時患有其他疾病或服用其他藥物,甚至有腎功能受損,也無須調校「利格列汀」的用藥劑量(「利格列汀」並非主要依靠腎臟排出體外)。
安全性與耐受性
「利格列汀」的整體副作用發生率與安慰劑相若,耐受性佳[10][11][12] [13][17]。即使單獨用藥或合併其他抗糖尿病藥物如甲福明、磺胺脲類或格列酮類,病人出現血糖過低的風險並無顯著增加。當與其他常用的抗糖尿病藥物合併治療,「利格列汀」亦無產生明顯的藥物相互作用,意味着不論病人是否患有其他疾病或同時服用其他常見的藥物,都適合接受「利格列汀」治療[18][19]。與磺胺脲類、 格列酮類或胰島素治療不同,「利格列汀」並不會引致體重上升,亦不會產生傳統抗糖尿病藥常見的副作用[20]。與許多傳統二型糖尿病治療相反,開始「利格列汀」治療時,病人無需經歷一段劑量調校期(即逐步增加劑量)以找出適當的治療劑量。
劑量
「利格列汀」的一般劑量是5毫克藥片。
不宜服用的人士
- 對「利格列汀」有效成分過敏
- 患有一型糖尿病
- 有糖尿病酮症酸中毒症
- 懷孕、正在授乳或準備授乳
副作用
研究証實少數服用者會出現血糖過低的情況,而極少數服用者會出現過敏的情況。
参考文献
- FDA approves new treatment for Type 2 diabetes. 3 May 2011. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm253501.htm (页面存档备份,存于). Accessed 25 February 2012.
- Blech S, Ludwig-Schwellinger E, Grafe-Mody EU, Withopf B, Wagner K. The metabolism and disposition of the oral dipeptidyl peptidase-4 inhibitor, linagliptin, in humans. Drug Metab Dispos 2010 Apr;38(4):667-678.
- Carolyn F Deacon, Jens J Holst. Dipeptidyl peptidase-4 inhibitors for the treatment of type 2 diabetes: comparison, efficacy and safety. Informa Healthcare Expert Opinion Reviews. October 2013, Vol. 14, No. 15 , Pages 2047-2058.
- Sitagliptin summary of product characteristics. Available at www.medicines.org.uk/emc/medicine/19609.
- Vildaliptin summary of product characteristics. Available at www.medicines.org.uk/emc/medicine/20734.
- Saxagliptin summary of product characteristics. Available at www.medicines.org.uk/EMC/medicine/22315.
- Thomas L, Tadayyon M, Mark M. Chronic treatment with the dipeptidyl peptidase-4 inhibitor BI 135 [(R)-8-(3-amino-piperidin-1-yl)-7-but-2-ynyl-3-methyl-1-(4-methyl-quinazol in-2-ylmethyl)-3,7-dihydro-purine-2,6-dione] increases basal glucagon-like peptide-1 and improves glycemic control in diabetic rodent models. J Pharmacol Exp Ther 2009;328(2):556-563.
- Barnett AJH, Harper R, Toorawa R, et al. Linagliptin monotherapy improves glycaemic control in type 2 diabetes patients for who metformin therapy is inappropriate. Poster No 823-P, 46th European Association for the Study of Diabetes Annual Meeting, 20-14 September 2010, Stockholm, Sweden.
- Lewin AJ, Arvay L, Liu D, et al. Safety and efficacy of linagliptin as add-on therapy to a sulphonylurea in inadequately controlled type 2 diabetes. Poster No 821-P, 46th European Association for the Study of Diabetes Annual Meeting, 20-14 September 2010, Stockholm, Sweden.
- Owens DR, Swallow R, Kugi KA, Woerle HJ. Efficacy and safety of linagliptin in persons with type 2 diabetes inadequately controlled by a combination of metformin and sulphonylurea: a 24-week randomized study. Diabet Med 2011;28(11):1352-1361.
- Taskinen M-R, et al. Efficacy and safety of linagliptin in Type 2 diabetes inadequately controlled on metformin monotherapy. Poster No 579-P from the 70th American Diabetes Association Scientific Sessions, 25-29 June 2010, Orlando, Florida, USA.
- Del Prato S, Barnett AH, Huisman H, et al. Effect of linagliptin monotherapy on glycaemic control and markers of β-cell function in patients with inadequately controlled type 2 diabetes: a randomized controlled trial. Diabetes Obes Metab 2011;13(3):258-267.
- Gomis R, Espadero RM, Jones R, Woerle HJ, Dugi KA. Efficacy and safety of initial combination therapy with linagliptin and pioglitazone in patients with inadequately controlled type 2 diabetes: a randomized, double-blind, placebo-controlled study. Diabetes Obes Metab 2011;13(7):653-661.
- Kawamori R, Inagaki N, Araki E, et al. Linagliptin monotherapy provides superior glycaemic control versus placebo or voglibose with comparable safety in Japanese patients with type 2 diabetes: a randomized, placebo and active comparator-controlled, double-blind study. Diabetes Obes Metab 2011;Dec 6 [Epub ahead of print].
- Kawamori R. et al. Linagliptin monotherapy improves glycemic control in Japanese patients with T2DM over 12 weeks. Poster number 696-P from the 70th American Diabetes Association Scientific Sessions, 25-29 June 2010, Orlando, Florida, USA
- Gallwitz B, Uhlig-Laske B, Bhattacharaya S, et al. Linagliptin has similar efficacy to glimepiride but improved cardiovascular safety over 2 years in patients with type 2 diabetes inadequately controlled on metformin 71th Scientific Sessions of the American Diabetes Association, San Diego, California. 2011; Poster 39-LB.
- Kawamori R. et al. Linagliptin monotherapy improves glycemic control in Japanese patients with T2DM over 12 weeks. Poster number 696-P from the 70th American Diabetes Association Scientific Sessions, 25-29 June 2010, Orlando, Florida, USA.
- Scheen AJ. Dipeptidylpeptidase-4 inhibitors (Gliptins). Clin Pharmacokinet 2010;49(9):573-588.
- Graefe-Mody U, Friedrich C, Port A, et al. Linagliptin, a novel DPP-4 inhibitor: no need for dose adjustment in patients with renal impairment. Poster No. 822-P, 46th European Association for the Study of Diabetes Annual Meeting, 20-24 September 2010, Stockholm, Sweden.
- Pratley R. Inhibition of DPP-4: a new therapeutic approach for the treatment of Type 2 diabetes. Curr Med Res Opin 2007;23(4):919-931.