
Atomoxetine, sold under the brand name Strattera, is a medication used to treat attention deficit hyperactivity disorder (ADHD)[12] and, to a lesser extent, cognitive disengagement syndrome.[13][14] It may be used alone or along with psychostimulants.[15][16] It is also used as a cognitive and executive functioning enhancer to improve self-motivation, persistence, attention, inhibition, and working memory.[17][18][19] Use of atomoxetine is only recommended for those who are at least six years old.[12] It is taken orally.[12] Atomoxetine is a selective norepinephrine reuptake inhibitor and is believed to work by increasing norepinephrine and dopamine levels in the brain.[12][10] The effectiveness of atomoxetine is comparable to the commonly prescribed stimulant medication methylphenidate.[20][21][22][23]
Common side effects of atomoxetine include abdominal pain, loss of appetite, nausea, feeling tired, and dizziness.[12] Serious side effects may include angioedema, liver problems, stroke, psychosis, heart problems, suicide, and aggression.[12][24] There is a lack of data regarding its safety during pregnancy; as of 2019, its safety during pregnancy and for use during breastfeeding is not certain.[25][26]
It was approved for medical use in the United States in 2002.[12] In 2020, it was the 287th most commonly prescribed medication in the United States, with more than 1 million prescriptions.[27][28]
Medical uses
Atomoxetine is indicated for the treatment of attention deficit hyperactivity disorder (ADHD).[5]
Attention deficit hyperactivity disorder
Atomoxetine is approved for use in children, adolescents, and adults.[5] However, its efficacy has not been studied in children under six years old.[8] One of the primary differences with the standard stimulant treatments for ADHD is that it has little known abuse potential.[8] Studies and meta-analyses indicate that atomoxetine has comparable efficacy and equal tolerability to methylphenidate in children and adolescents. In adults, efficacy and tolerability are equivalent.[20][21][22][23]
While its efficacy may be less than that of amphetamine,[29] there is some evidence that it may be used in combination with stimulants.[15] Doctors may prescribe non-stimulants including atomoxetine when a person has bothersome side effects from stimulants; when a stimulant was not effective; in combination with a stimulant to increase effectiveness;[30][31] when the cost of stimulants is prohibitive; or when there is concern about the abuse potential of psychostimulants in a patient with a history of drug use disorder.
Unlike α2 adrenoceptor agonists such as guanfacine and clonidine, atomoxetine's use can be abruptly stopped without significant discontinuation effects being seen.[8]
The initial therapeutic effects of atomoxetine usually take 1 to 4 weeks to become apparent.[7][32][33] A further 2 to 4 weeks may be required for the full therapeutic effects to be seen.[34][32] Incrementally increasing response may occur up to 1 year or longer.[33][35] The maximum recommended total daily dose in children and adolescents over 70 kg and adults is 100 mg.[5]
Other uses
Atomoxetine is sometimes used in the treatment of cognitive impairment and frontal lobe symptoms due to conditions like traumatic brain injury (TBI).[36][37] It is used with the goal of treating symptoms like attentional problems, lack of arousal, fatigue, and depression.[36] A 2015 Cochrane review identified only one study of atomoxetine for TBI and found no positive effects.[38] Aside from TBI, atomoxetine was found to be effective in the treatment of akinetic mutism following subarachnoid hemorrhage in a case report.[37][39]
Contraindications
Contraindications include:[8]
- Any cardiovascular disease including:
- Moderate to severe hypertension
- Atrial fibrillation
- Atrial flutter
- Ventricular tachycardia
- Ventricular fibrillation
- Ventricular flutter
- Advanced arteriosclerosis
- Severe cardiovascular disorders
- Uncontrolled hyperthyroidism
- Pheochromocytoma
- Concomitant treatment with monoamine oxidase inhibitors
- Narrow angle glaucoma
Adverse effects
Common side effects include abdominal pain, loss of appetite, nausea, feeling tired, and dizziness.[12] Serious side effects may include angioedema, liver problems, stroke, psychosis, heart problems, suicide, and aggression.[12][24] A 2020 meta-analysis found that atomoxetine was associated with anorexia, weight loss, and hypertension, rating it as a "potentially least preferred agent based on safety" for treating ADHD.[40][41] As of 2019, safety in pregnancy and breastfeeding is not clear;[25] a 2018 review stated that, "[b]ecause of lack of data, the treating physician should consider stopping atomoxetine treatment in women with ADHD during pregnancy."[26]
The U.S. Food and Drug Administration (FDA) has issued a black box warning for suicidal behavior/ideation.[9] Similar warnings have been issued in Australia.[8][42] Unlike stimulant medications, atomoxetine does not have abuse liability or the potential to cause withdrawal effects on abrupt discontinuation.[8][43]
Overdose
Atomoxetine is relatively non-toxic in overdose. Single-drug overdoses involving over 1500 mg of atomoxetine have not resulted in death.[8]
Interactions
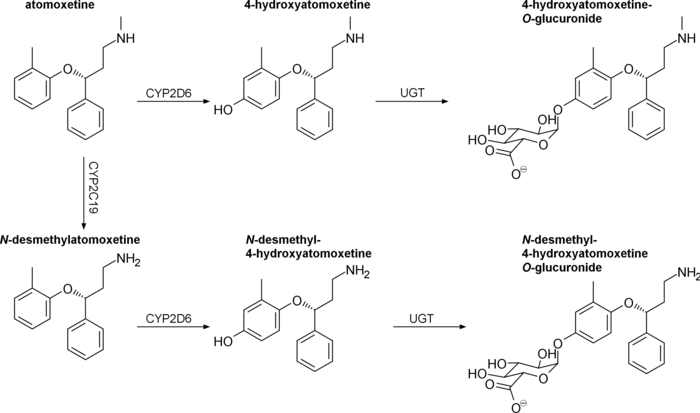
Atomoxetine is a substrate for CYP2D6. Concurrent treatment with a CYP2D6 inhibitor such as bupropion, fluoxetine, or paroxetine has been shown to increase plasma atomoxetine by 100% or more, as well as increase N-desmethylatomoxetine levels and decrease plasma 4-hydroxyatomoxetine levels by a similar degree.[44][45][46]
Atomoxetine has been found to directly inhibit hERG potassium currents with an IC50 of 6.3 μM, which has the potential to cause arrhythmia.[45][47] QT prolongation has been reported with atomoxetine at therapeutic doses and in overdose; it is suggested that atomoxetine not be used with other medications that may prolong the QT interval, concomitantly with CYP2D6 inhibitors, and caution to be used in poor metabolizers.[45]
Other notable drug interactions include:[8]
- Antihypertensive agents, due to atomoxetine acting as an indirect sympathomimetic
- Indirect-acting sympathomimetics, such as pseudoephedrine, norepinephrine reuptake inhibitors, or MAOIs
- Direct-acting sympathomimetics, such as phenylephrine or other α1 adrenoceptor agonists, including pressors such as dobutamine or isoprenaline and β2 adrenoceptor agonists
- Highly plasma protein-bound drugs: atomoxetine has the potential to displace these drugs from plasma proteins which may potentiate their adverse or toxic effects. In vitro, atomoxetine does not affect the plasma protein binding of aspirin, desipramine, diazepam, paroxetine, phenytoin, or warfarin[10][48]
Pharmacology
Pharmacodynamics
| Site | ATX | 4-OH-ATX | N-DM-ATX | |
|---|---|---|---|---|
| SERT | 77 | 43 | ND | |
| NET | 5 | 3 | 92 | |
| DAT | 1,451 | ND | ND | |
| 5-HT1A | >1,000 | ND | ND | |
| 5-HT1B | >1,000 | ND | ND | |
| 5-HT1D | >1,000 | ND | ND | |
| 5-HT2 | 2,000 | 1,000 | 1,700 | |
| 5-HT6 | >1,000 | ND | ND | |
| 5-HT7 | >1,000 | ND | ND | |
| α1 | 11,400 | 20,000 | 19,600 | |
| α2A | 29,800 | >30,000 | >10,000 | |
| β1 | 18,000 | 56,100 | 32,100 | |
| M1 | >100,000 | >100,000 | >100,000 | |
| M2 | >100,000 | >100,000 | >100,000 | |
| D1 | >10,000 | >10,000 | >10,000 | |
| D2 | >10,000 | >10,000 | >10,000 | |
| H1 | 12,100 | >100,000 | >100,000 | |
| MOR | ND | 422 | ND | |
| DOR | ND | 300 | ND | |
| KOR | ND | 95 | ND | |
| σ1 | >1,000 | ND | ND | |
| GABAA | 200 | >30,000 | >10,000 | |
| NMDA | 3,470a | ND | ND | |
| Kir3.1/3.2 | 10,900b | ND | ND | |
| Kir3.2 | 12,400b | ND | ND | |
| Kir3.1/3.4 | 6,500b | ND | ND | |
| hERG | 6,300 | 20,000 | 5,710 | |
| Values are Ki (nM). The smaller the value, the more strongly the drug binds to the site. All values are for human receptors unless otherwise specified. arat cortex. bXenopus oocytes. Additional sources:[51][52][10][48] | ||||
Atomoxetine inhibits the presynaptic norepinephrine transporter (NET), preventing the reuptake of norepinephrine throughout the brain along with inhibiting the reuptake of dopamine in specific brain regions such as the prefrontal cortex, where dopamine transporter (DAT) expression is minimal.[10] In rats, atomoxetine increased prefrontal cortex catecholamine concentrations without altering dopamine levels in the striatum or nucleus accumbens; in contrast, methylphenidate, a dopamine reuptake inhibitor, was found to increase prefrontal, striatal, and accumbal dopamine levels to the same degree.[51] In addition to rats, atomoxetine has also been found to induce similar region-specific catecholamine level alteration in mice.[53]
Atomoxetine's status as a serotonin transporter (SERT) inhibitor at clinical doses in humans is uncertain. A PET imaging study on rhesus monkeys found that atomoxetine occupied >90% and >85% of neural NET and SERT, respectively.[54] However, both mouse and rat microdialysis studies have failed to find an increase in extracellular serotonin in the prefrontal cortex following acute or chronic atomoxetine treatment.[51][53] Supporting atomoxetine's selectivity, a human study found no effects on platelet serotonin uptake (a marker of SERT inhibition) and inhibition of the pressor effects of tyramine (a marker of NET inhibition).[55]
Atomoxetine has been found to act as an NMDA receptor antagonist in rat cortical neurons at therapeutic concentrations.[56][57] It causes a use-dependent open-channel block and its binding site overlaps with the Mg2+ binding site.[56][57] Atomoxetine's ability to increase prefrontal cortex firing rate in anesthetized rats could not be blocked by D1 or α1-adrenergic receptor antagonists, but could be potentiated by NMDA or an α2-adrenergic receptor antagonist, suggesting a glutaminergic mechanism.[58] In Sprague Dawley rats, atomoxetine reduces NR2B protein content without altering transcript levels.[59] Aberrant glutamate and NMDA receptor function have been implicated in the etiology of ADHD.[60][61]
Atomoxetine also reversibly inhibits GIRK currents in Xenopus oocytes in a concentration-dependent, voltage-independent, and time-independent manner.[62] Kir3.1/3.2 ion channels are opened downstream of M2, α2, D2, and A1 stimulation, as well as other Gi-coupled receptors.[62] Therapeutic concentrations of atomoxetine are within range of interacting with GIRKs, especially in CYP2D6 poor metabolizers.[62] It is not known whether this contributes to the therapeutic effects of atomoxetine in ADHD.
4-Hydroxyatomoxetine, the major active metabolite of atomoxetine in CYP2D6 extensive metabolizers, has been found to have sub-micromolar affinity for opioid receptors, acting as an antagonist at μ-opioid receptors and a partial agonist at κ-opioid receptors.[52] It is not known whether this action at the kappa-opioid receptor leads to CNS-related adverse effects.
Pharmacokinetics
Orally administered atomoxetine is rapidly and completely absorbed.[10] First-pass metabolism by the liver is dependent on CYP2D6 activity, resulting in an absolute bioavailability of 63% for extensive metabolizers and 94% for poor metabolizers.[10] Maximum plasma concentration is reached in 1–2 hours.[10] If taken with food, the maximum plasma concentration decreases by 10-40% and delays the tmax by 3 hours.[10] Drugs affecting gastric pH have no effect on oral bioavailability.[5]
Following intravenous delivery, atomoxetine has a volume of distribution of 0.85 L/kg (indicating distribution primarily in total body water), with limited partitioning into red blood cells.[10][63] It is highly bound to plasma proteins (98.7%), mainly albumin, along with α1-acid glycoprotein (77%) and IgG (15%).[10][48] Its metabolite N-desmethylatomoxetine is 99.1% bound to plasma proteins, while 4-hydroxyatomoxetine is only 66.6% bound.[10]
The half-life of atomoxetine varies widely between individuals, with an average range of 4.5 to 19 hours.[10][11] As atomoxetine is metabolized by CYP2D6, exposure may be increased 10-fold in CYP2D6 poor metabolizers.[11] Among CYP2D6 extensive metabolizers, the half-life of atomoxetine averaged 5.34 hours and the half-life of the active metabolite N-desmethylatomoxetine was 8.9 hours.[10][64] By contrast, among CYP2D6 poor metabolizers the half-life of atomoxetine averaged 20.0 hours and the half-life of N-desmethylatomoxetine averaged 33.3 hours.[10][64] Steady-state levels of atomoxetine are typically achieved at or around day 10 of regular dosing, with trough plasma concentrations (Ctrough) residing around 30–40°ng/mL; however, both the time to steady-state levels and Ctrough are expected to vary based on a patient's CYP2D6 profile.[65][66]
Atomoxetine, N-desmethylatomoxetine, and 4-hydroxyatomoxetine produce minimal to no inhibition of CYP1A2 and CYP2C9, but inhibit CYP2D6 in human liver microsomes at concentrations between 3.6 and 17 μmol/L. Plasma concentrations of 4-hydroxyatomoxetine and N-desmethylatomoxetine at steady state are 1.0% and 5% that of atomoxetine in CYP2D6 extensive metabolizers, and are 5% and 45% that of atomoxetine in CYP2D6 poor metabolizers.[5]
Atomoxetine is excreted unchanged in urine at <3% in both extensive and poor CYP2D6 metabolizers, with >96% and 80% of a total dose being excreted in urine, respectively.[10] The fractions excreted in urine as 4-hydroxyatomoxetine and its glucuronide account for 86% of a given dose in extensive metabolizers, but only 40% in poor metabolizers.[10] CYP2D6 poor metabolizers excrete greater amounts of minor metabolites, namely N-desmethylatomoxetine and 2-hydroxymethylatomoxetine and their conjugates.[10]
Pharmacogenomics
Chinese adults homozygous for the hypoactive CYP2D6*10 allele have been found to exhibit two-fold higher area-under-the-curve (AUCs) and 1.5-fold higher maximum plasma concentrations compared to extensive metabolizers.[10]
Japanese men homozygous for CYP2D6*10 have similarly been found to experience two-fold higher AUCs compared to extensive metabolizers.[10]
Chemistry
Atomoxetine, or (−)-methyl[(3R)-3-(2-methylphenoxy)-3-phenylpropylamine, is a white, granular powder that is highly soluble in water.
 Strattera 60-mg capsule back
Strattera 60-mg capsule back Strattera 60-mg capsule front with Lilly logo
Strattera 60-mg capsule front with Lilly logo
Synthesis

Detection in biological fluids
Atomoxetine may be quantitated in plasma, serum or whole blood in order to distinguish extensive versus poor metabolizers in those receiving the drug therapeutically, to confirm the diagnosis in potential poisoning victims or to assist in the forensic investigation in a case of fatal overdosage.[69]
History
Atomoxetine is manufactured, marketed, and sold in the United States as the hydrochloride salt (atomoxetine HCl) under the brand name Strattera by Eli Lilly and Company, the original patent-filing company and current U.S. patent owner. Atomoxetine was initially intended to be developed as an antidepressant, but it was found to be insufficiently efficacious for treating depression. It was, however, found to be effective for ADHD and was approved by the FDA in 2002, for the treatment of ADHD. Its patent expired in May 2017.[70] On 12 August 2010, Lilly lost a lawsuit that challenged its patent on Strattera, increasing the likelihood of an earlier entry of a generic into the US market.[71] On 1 September 2010, Sun Pharmaceuticals announced it would begin manufacturing a generic in the United States.[72] In a 29 July 2011 conference call, however, Sun Pharmaceutical's Chairman stated "Lilly won that litigation on appeal so I think [generic Strattera]'s deferred."[73]
In 2017 the FDA approved the generic production of atomoxetine by four pharmaceutical companies.[74]
Society and culture
The drug was originally known as tomoxetine. It was renamed to avoid medication errors, as the name may be confused with tamoxifen.[75]
Brand names
In India, atomoxetine is sold under brand names including Axetra, Axepta, Attera, Tomoxetin, and Attentin. In Australia, Canada, Italy, Portugal, Romania, Spain, Switzerland and the US, atomoxetine is sold under the brand name Strattera. In the Czech Republic it is sold under brand names including Mylan. In Iran, atomoxetine is sold under brand names including Stramox. In 2017, a generic version was approved in the United States.[74]
Research
There has been some suggestion that atomoxetine might be a helpful adjunct in people with major depression, particularly in cases with concomitant ADHD.[76]
Atomoxetine may be used in those with ADHD and bipolar disorder although such use has not been well studied.[77] Some benefit has also been seen in people with ADHD and autism.[78] As with other norepinephrine reuptake inhibitors it appears to reduce anxiety and depression symptoms, although attention has focused mainly on specific patient groups such as those with concurrent ADHD[79] or methamphetamine dependence.[80]
Cognitive disengagement syndrome
Some studies indicate that atomoxetine is effective for treatment of cognitive disengagement syndrome.[13]
References
- ↑ "Atomoxetine (Strattera) Use During Pregnancy". Drugs.com. 22 August 2019. Archived from the original on 22 March 2019. Retrieved 7 February 2020.
- ↑ Anvisa (15 September 2023). "RDC Nº 816 - Listas de Substâncias Entorpecentes, Psicotrópicas, Precursoras e Outras sob Controle Especial" [Collegiate Board Resolution No. 816 - Lists of Narcotic, Psychotropic, Precursor, and Other Substances under Special Control] (in Brazilian Portuguese). Diário Oficial da União (published 18 September 2023). Archived from the original on 19 October 2023. Retrieved 19 October 2023.
- ↑ "Strattera 10mg hard capsules - Summary of Product Characteristics (SmPC)". (emc). 8 February 2021. Archived from the original on 8 October 2021. Retrieved 11 June 2022.
- ↑ "FDA-sourced list of all drugs with black box warnings (Use Download Full Results and View Query links.)". nctr-crs.fda.gov. FDA. Retrieved 22 October 2023.
- 1 2 3 4 5 6 "Strattera- atomoxetine hydrochloride capsule". DailyMed.gov. Eli Lilly and Company. 29 January 2020. Archived from the original on 7 June 2018. Retrieved 26 February 2020.
- ↑ "Active substance(s): atomoxetine" (PDF). List of nationally authorised medicinal products. European Medicines Agency. 2016. Archived (PDF) from the original on 12 June 2022. Retrieved 12 June 2022.
- 1 2 3 4 5 6 "atomoxetine (Rx) – Strattera". Medscape Reference. WebMD. Archived from the original on 10 November 2013. Retrieved 10 November 2013.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 "Strattera (atomoxetine hydrochloride)". TGA eBusiness Services. Eli Lilly Australia Pty. Limited. 21 August 2013. Archived from the original on 6 April 2017. Retrieved 10 November 2013.
- 1 2 3 4 5 6 "Atomoxetine Hydrochloride capsule [Mylan Pharmaceuticals Inc.]". DailyMed. Mylan Pharmaceuticals Inc. October 2011. Archived from the original on 10 November 2013. Retrieved 10 November 2013.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 Sauer JM, Ring BJ, Witcher JW (2005). "Clinical pharmacokinetics of atomoxetine". Clinical Pharmacokinetics. 44 (6): 571–590. doi:10.2165/00003088-200544060-00002. PMID 15910008. S2CID 25708096.
- 1 2 3 Brown JT, Bishop JR (2015). "Atomoxetine pharmacogenetics: associations with pharmacokinetics, treatment response and tolerability". Pharmacogenomics. 16 (13): 1513–1520. doi:10.2217/PGS.15.93. PMID 26314574.
- 1 2 3 4 5 6 7 8 9 "Atomoxetine Hydrochloride Monograph for Professionals". Drugs.com. American Society of Health-System Pharmacists. Archived from the original on 4 April 2019. Retrieved 22 March 2019.
- 1 2 McBurnett K, Clemow D, Williams D, Villodas M, Wietecha L, Barkley R (February 2017). "Atomoxetine-Related Change in Sluggish Cognitive Tempo Is Partially Independent of Change in Attention-Deficit/Hyperactivity Disorder Inattentive Symptoms". Journal of Child and Adolescent Psychopharmacology. 27 (1): 38–42. doi:10.1089/cap.2016.0115. PMID 27845858.
- ↑ Becker SP, Willcutt EG, Leopold DR, Fredrick JW, Smith ZR, Jacobson LA, et al. (June 2023). "Report of a Work Group on Sluggish Cognitive Tempo: Key Research Directions and a Consensus Change in Terminology to Cognitive Disengagement Syndrome". Journal of the American Academy of Child and Adolescent Psychiatry. 62 (6): 629–645. doi:10.1016/j.jaac.2022.07.821. PMC 9943858. PMID 36007816.
{{cite journal}}: CS1 maint: overridden setting (link) - 1 2 Treuer T, Gau SS, Méndez L, Montgomery W, Monk JA, Altin M, et al. (April 2013). "A systematic review of combination therapy with stimulants and atomoxetine for attention-deficit/hyperactivity disorder, including patient characteristics, treatment strategies, effectiveness, and tolerability". Journal of Child and Adolescent Psychopharmacology. 23 (3): 179–193. doi:10.1089/cap.2012.0093. PMC 3696926. PMID 23560600.
{{cite journal}}: CS1 maint: overridden setting (link) - ↑ "Parent's Medication Guide: ADHD". American Psychiatric Association (Guidelines (Tertiary source)). American Psychiatric Association & American Academy of Child and Adolescent Psychiatry (AACAP). June 2013. Archived from the original on 2 February 2017. Retrieved 1 January 2017.
Though not FDA-approved for combined treatment, atomoxetine (Strattera) is sometimes used in conjunction with stimulants as an off-label combination therapy.
- ↑ Malenka RC, Nestler EJ, Hyman SE, Holtzman DM (2015). "14: Higher Cognitive Function and Behavioral Control". Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (3 ed.). New York: McGraw-Hill Medical. ISBN 9780071827706.
- ↑ Chan E, Fogler JM, Hammerness PG (May 2016). "Treatment of Attention-Deficit/Hyperactivity Disorder in Adolescents: A Systematic Review". JAMA. 315 (18): 1997–2008. doi:10.1001/jama.2016.5453. PMID 27163988.
- ↑ Sofuoglu M, DeVito EE, Waters AJ, Carroll KM (January 2013). "Cognitive enhancement as a treatment for drug addictions". Neuropharmacology. 64 (1): 452–463. doi:10.1016/j.neuropharm.2012.06.021. PMC 3445733. PMID 22735770.
- 1 2 Hanwella R, Senanayake M, de Silva V (10 November 2011). "Comparative efficacy and acceptability of methylphenidate and atomoxetine in treatment of attention deficit hyperactivity disorder in children and adolescents: a meta-analysis". BMC Psychiatry. 11: 176. doi:10.1186/1471-244X-11-176. ISSN 1471-244X. PMC 3229459. PMID 22074258.
- 1 2 Rezaei G, Hosseini SA, Akbari Sari A, Olyaeemanesh A, Lotfi MH, Yassini M, et al. (10 February 2016). "Comparative efficacy of methylphenidate and atomoxetine in the treatment of attention deficit hyperactivity disorder in children and adolescents: A systematic review and meta-analysis". Medical Journal of the Islamic Republic of Iran. 30: 325. PMC 4898838. PMID 27390695.
{{cite journal}}: CS1 maint: overridden setting (link) - 1 2 Hazell PL, Kohn MR, Dickson R, Walton RJ, Granger RE, van Wyk GW (November 2011). "Core ADHD Symptom Improvement With Atomoxetine Versus Methylphenidate: A Direct Comparison Meta-Analysis". Journal of Attention Disorders. 15 (8): 674–683. doi:10.1177/1087054710379737. ISSN 1087-0547. PMID 20837981. S2CID 43503227. Archived from the original on 15 November 2023. Retrieved 7 December 2023.
- 1 2 Bushe C, Day K, Reed V, Karlsdotter K, Berggren L, Pitcher A, et al. (May 2016). "A network meta-analysis of atomoxetine and osmotic release oral system methylphenidate in the treatment of attention-deficit/hyperactivity disorder in adult patients". Journal of Psychopharmacology. 30 (5): 444–458. doi:10.1177/0269881116636105. ISSN 0269-8811. PMID 27005307. S2CID 104938. Archived from the original on 23 May 2023. Retrieved 7 December 2023.
- 1 2 British national formulary : BNF 76 (76 ed.). Pharmaceutical Press. 2018. pp. 344–345. ISBN 9780857113382.
- 1 2 "Atomoxetine Pregnancy and Breastfeeding Warnings". Drugs.com. Archived from the original on 22 March 2019. Retrieved 3 March 2019.
- 1 2 Ornoy A (February 2018). "Pharmacological Treatment of Attention Deficit Hyperactivity Disorder During Pregnancy and Lactation". Pharmaceutical Research (Review). 35 (3): 46. doi:10.1007/s11095-017-2323-z. PMID 29411149. S2CID 3663423.
- ↑ "The Top 300 of 2020". ClinCalc. Archived from the original on 14 May 2020. Retrieved 7 October 2022.
- ↑ "Atomoxetine - Drug Usage Statistics". ClinCalc. Archived from the original on 7 October 2021. Retrieved 7 October 2022.
- ↑ Kooij JJ (2013). Adult ADHD Diagnostic Assessment and Treatment. Springer London. doi:10.1007/978-1-4471-4138-9. ISBN 978-1-4471-4137-2. S2CID 51698077.
- ↑ "Attention Deficit Hyperactivity Disorder". National Institute of Mental Health (NIMH). Archived from the original on 25 December 2016. Retrieved 21 July 2018.
- ↑ "Mental Health Medications". NIMH. Archived from the original on 6 April 2019. Retrieved 17 May 2019.
- 1 2 Bushe CJ, Savill NC (March 2014). "Systematic review of atomoxetine data in childhood and adolescent attention-deficit hyperactivity disorder 2009-2011: focus on clinical efficacy and safety". J Psychopharmacol. 28 (3): 204–11. doi:10.1177/0269881113478475. PMID 23438503. S2CID 793033.
- 1 2 Childress AC (2016). "A critical appraisal of atomoxetine in the management of ADHD". Ther Clin Risk Manag. 12: 27–39. doi:10.2147/TCRM.S59270. PMC 4694693. PMID 26730199.
- ↑ Taylor D, Paton C, Shitij K (2012). The Maudsley prescribing guidelines in psychiatry. West Sussex: Wiley-Blackwell. ISBN 978-0-470-97948-8.
- ↑ Clemow DB, Bushe CJ (December 2015). "Atomoxetine in patients with ADHD: A clinical and pharmacological review of the onset, trajectory, duration of response and implications for patients". J Psychopharmacol. 29 (12): 1221–30. doi:10.1177/0269881115602489. PMID 26349559. S2CID 22649093.
- 1 2 Ripley DL (2006). "Atomoxetine for individuals with traumatic brain injury". J Head Trauma Rehabil. 21 (1): 85–8. doi:10.1097/00001199-200601000-00010. PMID 16456396.
- 1 2 Arnts H, van Erp WS, Lavrijsen JC, van Gaal S, Groenewegen HJ, van den Munckhof P (May 2020). "On the pathophysiology and treatment of akinetic mutism". Neurosci Biobehav Rev. 112: 270–278. doi:10.1016/j.neubiorev.2020.02.006. hdl:2066/225901. PMID 32044373. S2CID 211053123.
- ↑ Dougall D, Poole N, Agrawal N (December 2015). "Pharmacotherapy for chronic cognitive impairment in traumatic brain injury". Cochrane Database Syst Rev (12): CD009221. doi:10.1002/14651858.CD009221.pub2. PMID 26624881.
- ↑ Kim YW, Shin JC, An YS (July 2010). "Treatment of chronic akinetic mutism with atomoxetine: subtraction analysis of brain f-18 fluorodeoxyglucose positron emission tomographic images before and after medication: a case report". Clin Neuropharmacol. 33 (4): 209–11. doi:10.1097/WNF.0b013e3181dca948. PMID 20661027.
- ↑ Solmi M, Fornaro M, Ostinelli EG, Zangani C, Croatto G, Monaco F, et al. (June 2020). "Safety of 80 antidepressants, antipsychotics, anti-attention-deficit/hyperactivity medications and mood stabilizers in children and adolescents with psychiatric disorders: a large scale systematic meta-review of 78 adverse effects". World Psychiatry (Meta-analysis). 19 (2): 214–232. doi:10.1002/wps.20765. PMC 7215080. PMID 32394557.
{{cite journal}}: CS1 maint: overridden setting (link) - ↑ "Psychiatric drugs given to children and adolescents have been ranked in order of safety". NIHR Evidence (Plain English summary). 1 September 2020. doi:10.3310/alert_40795. S2CID 241309451. Archived from the original on 21 January 2022. Retrieved 12 March 2022.
- ↑ "Atomoxetine and suicidality in children and adolescents". Australian Prescriber. 4 (5): 166. October 2013. Archived from the original on 30 March 2015. Retrieved 10 November 2013.
- ↑ Wernicke JF, Adler L, Spencer T, West SA, Allen AJ, Heiligenstein J, et al. (February 2004). "Changes in symptoms and adverse events after discontinuation of atomoxetine in children and adults with attention deficit/hyperactivity disorder: a prospective, placebo-controlled assessment". Journal of Clinical Psychopharmacology. 24 (1): 30–35. doi:10.1097/01.jcp.0000104907.75206.c2. PMID 14709944. S2CID 37636280.
{{cite journal}}: CS1 maint: overridden setting (link) - ↑ Todor I, Popa A, Neag M, Muntean D, Bocsan C, Buzoianu A, et al. (April–June 2016). "Evaluation of a Potential Metabolism-Mediated Drug-Drug Interaction Between Atomoxetine and Bupropion in Healthy Volunteers". Journal of Pharmacy & Pharmaceutical Sciences. 19 (2): 198–207. doi:10.18433/j3h03r. PMID 27518170.
{{cite journal}}: CS1 maint: overridden setting (link) - 1 2 3 Kasi PM, Mounzer R, Gleeson GH (2011). "Cardiovascular side effects of atomoxetine and its interactions with inhibitors of the cytochrome p450 system". Case Reports in Medicine. 2011: 952584. doi:10.1155/2011/952584. PMC 3135225. PMID 21765848.
- ↑ Belle DJ, Ernest CS, Sauer JM, Smith BP, Thomasson HR, Witcher JW (November 2002). "Effect of potent CYP2D6 inhibition by paroxetine on atomoxetine pharmacokinetics". Journal of Clinical Pharmacology. 42 (11): 1219–27. doi:10.1177/009127002762491307. PMID 12412820. S2CID 40283275.
- ↑ Scherer D, Hassel D, Bloehs R, Zitron E, von Löwenstern K, Seyler C, et al. (January 2009). "Selective noradrenaline reuptake inhibitor atomoxetine directly blocks hERG currents". British Journal of Pharmacology. 156 (2): 226–36. doi:10.1111/j.1476-5381.2008.00018.x. PMC 2697834. PMID 19154426.
{{cite journal}}: CS1 maint: overridden setting (link) - 1 2 3 "21-411 Strattera Clinical Pharmacology Biopharmaceutics Review Part 2" (PDF). U.S. Food and Drug Administration (FDA). Archived (PDF) from the original on 1 March 2017. Retrieved 6 August 2017.
- ↑ Roth BL, Driscol J. "PDSP Ki Database". Psychoactive Drug Screening Program (PDSP). University of North Carolina at Chapel Hill and the United States National Institute of Mental Health. Archived from the original on 27 August 2021. Retrieved 14 August 2017.
- ↑ Upadhyaya HP, Desaiah D, Schuh KJ, Bymaster FP, Kallman MJ, Clarke DO, et al. (March 2013). "A review of the abuse potential assessment of atomoxetine: a nonstimulant medication for attention-deficit/hyperactivity disorder". Psychopharmacology. Springer Nature. 226 (2): 189–200. doi:10.1007/s00213-013-2986-z. PMC 3579642. PMID 23397050.
{{cite journal}}: CS1 maint: overridden setting (link) - 1 2 3 Bymaster FP, Katner JS, Nelson DL, Hemrick-Luecke SK, Threlkeld PG, Heiligenstein JH, et al. (November 2002). "Atomoxetine increases extracellular levels of norepinephrine and dopamine in prefrontal cortex of rat: a potential mechanism for efficacy in attention deficit/hyperactivity disorder". Neuropsychopharmacology. 27 (5): 699–711. doi:10.1016/S0893-133X(02)00346-9. PMID 12431845.
{{cite journal}}: CS1 maint: overridden setting (link) - 1 2 Creighton CJ, Ramabadran K, Ciccone PE, Liu J, Orsini MJ, Reitz AB (August 2004). "Synthesis and biological evaluation of the major metabolite of atomoxetine: elucidation of a partial kappa-opioid agonist effect". Bioorganic & Medicinal Chemistry Letters. 14 (15): 4083–5. doi:10.1016/j.bmcl.2004.05.018. PMID 15225731.
- 1 2 Koda K, Ago Y, Cong Y, Kita Y, Takuma K, Matsuda T (July 2010). "Effects of acute and chronic administration of atomoxetine and methylphenidate on extracellular levels of noradrenaline, dopamine and serotonin in the prefrontal cortex and striatum of mice". Journal of Neurochemistry. 114 (1): 259–70. doi:10.1111/j.1471-4159.2010.06750.x. PMID 20403082.
- ↑ Ding YS, Naganawa M, Gallezot JD, Nabulsi N, Lin SF, Ropchan J, et al. (February 2014). "Clinical doses of atomoxetine significantly occupy both norepinephrine and serotonin transports: Implications on treatment of depression and ADHD". NeuroImage. 86: 164–71. doi:10.1016/j.neuroimage.2013.08.001. PMID 23933039. S2CID 16958660.
The noradrenergic action also exerts an important clinical effect in different antidepressant classes such as desipramine and nortriptyline (tricyclics, prevalent noradrenergic effect), reboxetine and atomoxetine (relatively pure noradrenergic reuptake inhibitor (NRIs)), and dual action antidepressants such as the serotonin noradrenaline reuptake inhibitors (SNRIs), the noradrenergic and dopaminergic reuptake inhibitor (NDRI) bupropion, and other compounds (e.g., mianserin, mirtazapine), which enhance the noradrenergic transmission
{{cite journal}}: CS1 maint: overridden setting (link) - ↑ Zerbe RL, Rowe H, Enas GG, Wong D, Farid N, Lemberger L (January 1985). "Clinical pharmacology of tomoxetine, a potential antidepressant". The Journal of Pharmacology and Experimental Therapeutics. 232 (1): 139–43. PMID 3965689.
- 1 2 Ludolph AG, Udvardi PT, Schaz U, Henes C, Adolph O, Weigt HU, et al. (May 2010). "Atomoxetine acts as an NMDA receptor blocker in clinically relevant concentrations". British Journal of Pharmacology. 160 (2): 283–91. doi:10.1111/j.1476-5381.2010.00707.x. PMC 2874851. PMID 20423340.
{{cite journal}}: CS1 maint: overridden setting (link) - 1 2 Barygin OI, Nagaeva EI, Tikhonov DB, Belinskaya DA, Vanchakova NP, Shestakova NN (April 2017). "Inhibition of the NMDA and AMPA receptor channels by antidepressants and antipsychotics". Brain Research. 1660: 58–66. doi:10.1016/j.brainres.2017.01.028. PMID 28167075. S2CID 27647092.
- ↑ Di Miceli M, Gronier B (June 2015). "Psychostimulants and atomoxetine alter the electrophysiological activity of prefrontal cortex neurons, interaction with catecholamine and glutamate NMDA receptors". Psychopharmacology. 232 (12): 2191–205. doi:10.1007/s00213-014-3849-y. PMID 25572531. S2CID 18339166.
- ↑ Udvardi PT, Föhr KJ, Henes C, Liebau S, Dreyhaupt J, Boeckers TM, et al. (2013). "Atomoxetine affects transcription/translation of the NMDA receptor and the norepinephrine transporter in the rat brain--an in vivo study". Drug Design, Development and Therapy. 7: 1433–46. doi:10.2147/DDDT.S50448. PMC 3857115. PMID 24348020.
- ↑ Maltezos S, Horder J, Coghlan S, Skirrow C, O'Gorman R, Lavender TJ, et al. (March 2014). "Glutamate/glutamine and neuronal integrity in adults with ADHD: a proton MRS study". Translational Psychiatry. 4 (3): e373. doi:10.1038/tp.2014.11. PMC 3966039. PMID 24643164.
{{cite journal}}: CS1 maint: overridden setting (link) - ↑ Chang JP, Lane HY, Tsai GE (2014). "Attention deficit hyperactivity disorder and N-methyl-D-aspartate (NMDA) dysregulation". Current Pharmaceutical Design. 20 (32): 5180–5. doi:10.2174/1381612819666140110115227. PMID 24410567.
- 1 2 3 Kobayashi T, Washiyama K, Ikeda K (June 2010). "Inhibition of G-protein-activated inwardly rectifying K+ channels by the selective norepinephrine reuptake inhibitors atomoxetine and reboxetine". Neuropsychopharmacology. 35 (7): 1560–9. doi:10.1038/npp.2010.27. PMC 3055469. PMID 20393461.
- ↑ "atomoxetine HC" (PDF). FDA. Archived (PDF) from the original on 18 October 2023. Retrieved 30 November 2023.
- 1 2 Sauer JM, Ponsler GD, Mattiuz EL, Long AJ, Witcher JW, Thomasson HR, et al. (January 2003). "Disposition and metabolic fate of atomoxetine hydrochloride: the role of CYP2D6 in human disposition and metabolism". Drug Metabolism and Disposition. 31 (1): 98–107. doi:10.1124/dmd.31.1.98. PMID 12485958. S2CID 13032441.
- ↑ Sauer JM, Ring BJ, Witcher JW (2005). "Clinical pharmacokinetics of atomoxetine". Clinical Pharmacokinetics. 44 (6): 571–590. doi:10.2165/00003088-200544060-00002. PMID 15910008. S2CID 25708096.
- ↑ Chamberlain SR, Sahakian BJ (2010). "Atomoxetine". In Stolerman IP (ed.). Encyclopedia of Psychopharmacology. Berlin, Heidelberg: Springer. pp. 158–160. doi:10.1007/978-3-540-68706-1_35. ISBN 978-3-540-68706-1.
- ↑ A US patent 4018895 A, Bryan B. Molloy & Klaus K. Schmiegel, "Aryloxyphenylpropylamines in treating depression", published 19 April 1977, assigned to Eli Lilly And Company
- ↑ B1 US patent EP0052492 B1, Bennie Joe Foster & Edward Ralph Lavagnino, "3-aryloxy-3-phenylpropylamines", published 29 February 1984, assigned to Eli Lilly And Company
- ↑ Baselt RC (2008). Disposition of Toxic Drugs and Chemicals in Man (8th ed.). Foster City, CA: Biomedical Publications. pp. 118–20. ISBN 978-0-931890-08-6.
- ↑ "Patent and Exclusivity Search Results". Electronic Orange Book. U.S. Food and Drug Administration (FDA). Archived from the original on 22 March 2012. Retrieved 26 April 2009.
- ↑ "Drugmaker Eli Lilly loses patent case over ADHD drug, lowers revenue outlook". Chicago Tribune.
- ↑ "Sun Pharma receives USFDA approval for generic Strattera capsules". International Business Times. Archived from the original on 7 April 2011.
- ↑ "Sun Pharma Q1 2011-12 Earnings Call Transcript 10.00 am, July 29, 2011" (PDF). Archived from the original (PDF) on 29 September 2011.
- 1 2 "FDA approves first generic Strattera for the treatment of ADHD". U.S. Food and Drug Administration (FDA) (Press release). 30 May 2017. Archived from the original on 4 June 2017. Retrieved 1 January 2018.
- ↑ Ledbetter M (December 2006). "Atomoxetine: a novel treatment for child and adult ADHD". Neuropsychiatric Disease and Treatment. 2 (4): 455–466. doi:10.2147/nedt.2006.2.4.455. PMC 2671957. PMID 19412494.
- ↑ Malenka RC, Nestler EJ, Hyman SE, Holtzman DM (2015). Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (3rd ed.). New York: McGraw-Hill Medical. ISBN 9780071827706.
- ↑ Perugi G, Vannucchi G (2015). "The use of stimulants and atomoxetine in adults with comorbid ADHD and bipolar disorder". Expert Opinion on Pharmacotherapy. 16 (14): 2193–204. doi:10.1517/14656566.2015.1079620. PMID 26364896. S2CID 28907560.
- ↑ Siegel M, Erickson C, Frazier JA, Ferguson T, Goepfert E, Joshi G, et al. (Autism Society of America) (2016). Autism Spectrum Disorder Parents Medication Guide (PDF). Washington, DC: American Academy of Child and Adolescent Psychiatry. p. 13. Archived (PDF) from the original on 11 April 2017.
Atomoxetine (Strattera) has also been researched in controlled studies for treatment of ADHD in children with autism, and showed some improvements, particularly for hyperactivity and impulsivity
- ↑ Snircova E, Marcincakova-Husarova V, Hrtanek I, Kulhan T, Ondrejka I, Nosalova G (June 2016). "Anxiety reduction on atomoxetine and methylphenidate medication in children with ADHD". Pediatrics International. 58 (6): 476–81. doi:10.1111/ped.12847. PMID 26579704. S2CID 6229741.
- ↑ Rabiey A, Hassani-Abharian P, Farhad M, Moravveji AR, Akasheh G, Banafshe HR (December 2019). "Atomoxetine Efficacy in Methamphetamine Dependence during Methadone Maintenance Therapy". Archives of Iranian Medicine. 22 (12): 692–698. PMID 31823620.
Further reading
- Dean L (2015). "Atomoxetine Therapy and CYP2D6 Genotype". In Pratt VM, McLeod HL, Rubinstein WS, et al. (eds.). Medical Genetics Summaries. National Center for Biotechnology Information (NCBI). PMID 28520366. Bookshelf ID: NBK315951. Archived from the original on 26 October 2020. Retrieved 7 February 2020.